This is a guest post byKarissa Hansen, Ph.D. Candidate, UCSF Developmental and Stem Cell Biology (DSCB) Program
During class this week, one major topic of conversation was the forced sterilization of incarcerated individuals in California, often people of color, along with the eugenic principles that this thinking perpetuates. Dr. James Heinrich, an OB-GYN at one of these prisons, was quoted in an NPR article1 claiming that the amount of money spent on these procedures was minimal “compared to what you save in welfare paying for these unwanted children–as they procreated more.” My jaw dropped when I read this horribly prejudiced statement. Every individual is entitled to personal bodily autonomy. Although he appears to be referring to surgeries that were completed voluntarily, when a person in a powerless position is under coercive pressure, there clearly cannot be consent.
Although the forced sterilizations in the prison system being discussed are said to have occurred between the years of 2006-2010, such atrocities were occurring long before and continue today. In September 2020, a nurse working at a US Immigration and Customs Enforcement center in Georgia alleged that detained women were undergoing similar procedures, including unnecessary hysterectomies2. As of December, more than 40 individuals had submitted written testimony in a legal petition against the facility3.
So where do we go from here? I don’t have a good answer. Shutting down one problematic facility doesn’t prevent such procedures from happening at a dozen more. We are clearly unable to rid this system of the discriminatory beliefs it was built upon. As we’ve discussed, the roots of the issue must be addressed—and there are many.
This is a guest post byCambria Chou-Freed, Ph.D. Candidate, UCSF Biomedical Sciences (BMS) Program
This week, I was very interested in our class discussions about how race is used as a variable in medicine/biomedical research and about the contexts in which this might exacerbate vs. combat health inequities. I especially appreciated the UCSF debates over the use of genetic ancestry vs. race in eGFR and polygenic risk score calculations. What stuck with me was the question: how can we, as scientists and physicians, feel comfortable using race as a variable in the same way we use quantitative, measurable variables (ex: blood cell or RNA transcript counts) to make research claims and clinical diagnoses? We know that race is an inaccurate proxy for genetic ancestry in many cases. Furthermore, when we want to use race as a proxy for social factors, I wonder whether in the future we will move toward incorporating other, more precise variables instead (such as to what degree a person experiences racism in their life, or what neighborhood they live in, an example given in class). As a mixed-race person, it has always made intuitive sense to me that race is not clearly defined or discrete, even when I didn’t have the words or data to back this up. Similarly to what Dr. Grubbs argued in the debate, I wonder how researchers would calculate my risk for polygenic diseases if I don’t fit accurately or precisely into their race-based model?
Another question that came up in class is how epigenetics might be used in medicine/biomedical research. Epigenetic marks are thought to encode experiences and environmental factors such as trauma and stress at the molecular level, and there is evidence that epigenetic changes to DNA can be passed on through multiple generations. Many people see epigenetics as an opportunity to study the effects of social factors such as racism on human health, and I certainly see the potential benefits of this. However, I also worry that some people will use epigenetics as the next generation of scientific evidence to back the claim of “biological differences due to race” and that a new form of discrimination could emerge as a result.
This is a guest post byLauraAnn Schmidberger, Ph.D. Candidate, UCSF Tetrad Graduate Program
Assuming that the color of someone’s skin explains their life history seems ridiculous when it’s phrased that way, but it is easy to see how doctors can fall into the trap of using racial categories in their practice, especially given the pressure to assess their patients quickly. This article made me think of racial profiling—it is understandable that authorities would want a quick way to identify potential suspects, but to conflate race with the likelihood of committing a crime is inappropriate. Race is a much less important factor in both community safety and medicine than socioeconomic, geographic, and familial backgrounds. The author makes it clear that while taking the time to understand a patient’s background may not be as rapid, it is ultimately more efficient, because it will lead to fewer misdiagnoses. False assumptions about a patient’s condition based on their outward appearance increases the time it takes for an accurate diagnosis, which in the worst cases can be deadly. A country largely segregated by not only race but also geography and socioeconomic status became a country in which the three were conflated and each race was assumed homogenous, when in reality our communities have never been more diverse. Each person has a unique background, and “if a physician simply diagnoses ‘race,’” that background, including “environmental exposures, family histories, the stress of dealing with racism, access to and quality of care [,] may be left unexamined.”
This is a guest post byMariko Foecke, Ph.D. Candidate, UCSF Biomedical Sciences (BMS) Program & Eliza Gaylord, Ph.D. Candidate, UCSF Developmental and Stem Cell Biology (DSCB) Program
Despite the profound advancements achieved by modern medicine, people with ovaries in the United States were at a 10% greater risk of dying from a pregnancy-related death (PRD) in 2017 than they were in 19871. Strikingly, this risk is even greater for the BIPOC community, as Black people with ovaries account for 41.7% of PRDs. This statistic is three times higher than PRD rates for White people with ovaries1. The Centers for Disease Control defines a PRD as “the death of a woman during pregnancy or within one year of the end of pregnancy from a pregnancy complication; a chain of events initiated by pregnancy; or the aggravation of an unrelated condition by the physiologic effects of pregnancy”2.
Recent research highlights variables that may contribute to disparities in PRDs for people of color, such as quality of and access to care, implicit bias, and psychological stress induced by structural racism1. Examination of disparities in PRDs across socioeconomic and educational backgrounds identified that African Americans with ovaries with at least a college degree were 5.2 times more likely to suffer a PRD than White people with ovaries with the same level of education. Furthermore, the mortality rate of infants of college-educated African American people with ovaries was 3.1 times higher than infants of high school or less-educated White people with ovaries3. Thus, as disparities in PRD and infant mortality rates continue to rise, there is a critical need to understand the physiological impact of social determinants of health during pregnancy and their potentially multigenerational effects.
African Americans with ovaries experience high levels of physiological stress due to social discrimination and systemic racism4. Additionally, racial discrimination is directly correlated with higher levels of depression14, a known consequence of stress15. For decades, it has been appreciated anecdotally that both pre-pregnancy and maternal stress contribute to adverse health and infant birth outcomes5. Maternal stress during pregnancy may lead to high blood pressure and changes in dietary intake, increasing the risk for gestational diabetes, preterm labor, and preeclampsia16. Additionally, exposure to physiological stress after pregnancy may lead to postpartum depression or substance abuse17, accounting for an estimated 14% – 30% of reported maternal deaths18.
Concurrently, recent research has gleaned insights into the mechanisms underlying how the negative effects of maternal stress may persist for up to three generations6-8. In response to stress, fertility is known to decline as a consequence of a diminished ovarian reserve, which encompasses the quantity and quality of ovarian egg cells, or oocytes9,10. The incidence of oocyte aneuploidy, referring to an abnormal number of chromosomes, increases in response to maternal stress and is a known cause of infertility and disease11. Importantly, of the 10% of individuals with ovaries who struggle with fertility in the United States, 15% of them are affected by oocyte aneuploidy12. In fact, aneuploidy occurs in 5% of all clinically recognized pregnancies and is causal in 1 in 3 miscarriages13.
As the connection between physiological stress and poor health and infant outcomes, particularly for Black women, become increasingly clear, there is a dire need for immediate and effective action to close the persistent PRD and infant mortality gaps. In addition to implementing policy designed to protect vulnerable populations from stressful, discriminatory experiences in professional and higher education environments3, implicit bias training for healthcare professionals should be required to decrease disparities in prenatal and postpartum care19. Finally, legislation to provide federal support that increases access to mental health care and social services specifically to people of color with ovaries before, during, and after pregnancy19 is necessary to reduce this devastating maternal health crisis.
Bibliography:
Pregnancy Mortality Surveillance System. Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion. (2019).
Racial and Ethnic Disparities Continue in Pregnancy-Related Deaths. Centers for Disease Control and Prevention. (2019).
Fishman SH, Hummer RA, Sierra G, Hargrove T, Powers DA, Rogers RG. Race/ethnicity, maternal educational attainment, and infant mortality in the United States. Biodemography Soc Biol. (2020).
Howard JT, Sparks PJ. The role of education in explaining racial/ethnic allostatic load differentials in the United States. Biodemography Soc Biol. (2015).
Dole N, Savitz DA, Hertz-Picciotto I, Siega-Riz AM, McMahon MJ, Buekens P. Maternal stress and preterm birth. Am J Epidemiol. (2003).
Crews D, Gillette R, Scarpino SV, Manikkam M, Savenkova MI, Skinner MK. Epigenetic transgenerational inheritance of altered stress responses. Proc Natl Acad Sci U S A. (2012).
Ward ID, Zucchi FC, Robbins JC, et al. Transgenerational programming of maternal behaviour by prenatal stress. BMC Pregnancy Childbirth. (2013).
Kiss D, Ambeskovic M, Montina T. et al. Stress transgenerationally programs metabolic pathways linked to altered mental health. Cell. Mol. Life Sci. (2016).
De Felici M, Klinger FG, Farini D, Scaldaferri ML, Iona S, Lobascio M. Establishment of oocyte population in the fetal ovary: primordial germ cell proliferation and oocyte programmed cell death. Reprod Biomed Online. (2005).
Mikwar M, MacFarlane AJ, Marchetti F. Mechanisms of oocyte aneuploidy associated with advanced maternal age. Mutat Res. (2020).
Eisenberg E, Brumbaugh K, Brown-Bryant R, Warner L. Health topics: infertility. Office on Women’s Health in the U.S. Department of Health and Human Services. (2019).
Hassold T, Hunt P. To err (meiotically) is human: the genesis of human aneuploidy. Nat Rev Genet. (2001).
Hudson DL, Puterman E, Bibbins-Domingo K, Matthews KA, Adler NE. Race, life course socioeconomic position, racial discrimination, depressive symptoms and self-rated health. Soc Sci Med. (2013).
van Praag HM. Can stress cause depression? World J Biol Psychiatry. (2005).
Stress and Pregnancy. March of Dimes. (2019).
Postpartum Depression. Office on Women’s Health in the U.S. Department of Health and Human Services. (2019).
Maternal Mortality May Be Even Higher Than We Thought. Columbia University Irving Medical Center. (2019).
Bailey SR. Our Black maternal health crisis is an American tragedy. American Medical Association. (2021).
This is a guest post byJackie Roger, Ph.D. Candidate, UCSF Program in Bioinformatics (BI)
Towards the end of this past week, several of the readings and videos discussed the intersection of racism and OB-GYN. We learned about the medical experimentation on black women’s bodies (Linda Villarosa’s article in NYT), the mutilation and subsequent museum display of Sara Baartman’s genitalia (Dr. Deirdre Cooper Owens’s talk on Youtube), and the black maternal health crisis (Dr. Susan R. Bailey article on the AMA site). These examples illustrate how the historical legacies of anti-black racism are embedded in present-day OB-GYN research and medicine. One component of this is disparities in the maternal mortality rate, which was the focus of Dr. Bailey’s piece.
She described two initiatives to reduce this disparity: the MOMMA Act to extend coverage for post-partum care and the Release the Pressure campaign to promote heart health and healthy blood pressure. The MOMMA Act seems like a good start, and could reduce both overall maternal mortalities and the racial disparities in maternal mortalities. The Release the Pressure campaign calls upon black people to take steps in their own lives to improve their heart health (since heart disease is one of the leading causes of pregnancy-related death). There are so many aspects of systemic anti-black racism within the medical system and beyond that directly contribute to increased risk of heart disease. A campaign that asks them to offset these things by “taking a few more steps a day” etc seems insulting. I think that truly addressing disparities in OB-GYN will require structural changes in the healthcare system.
This is a guest post by Aris Tay, PhD Candidate, Bruce Wang and Diana Laird Labs, Developmental and Stem Cell Biology (DSCB), UCSF
In session 3 of UCSF’s racism and race: the use of race in medicine and implications for health equity discussion, as well as many other works centered around race in medicine, it was mentioned that race, as we use it colloquially, is a social construct. Due to my own identity, I often think about how gender is a social construct and how scientists often use the two terms sex and gender to separate out what is and is not scientifically and empirically biological and hard-wired. However, until this course I had not made the connection that race and racial identity is a social construct just like how gender is.
In many large scale observational genetic studies, specific genetic signatures (typically single nucleotide polymorphisms) are often found to be associated and even predicative for certain diseases. These genetic signatures are often correlated with self-identified racial groups. Thus, the field has often incorrectly assumed that race causes these genetic signatures which leads to a predisposition for disease, and that this is why I often hear statements such as “Tay-Sachs is most common is Ashkenazi Jews” or “Sickle cell anemia is more common in black people”. However, it is difficult, in these large observational studies, to separate lifestyle, family history, etc from the check box self-identified categories that patients are asked to bin themselves into. Self-identified categories of gender and race are much easier to draw correlations from; however, it is now coming to light that detailed family history and lifestyle is much more accurate. Social constructs of gender and race often make up core aspects of someone’s identify. This will definitely affect one’s choices and lifestyle which could then affect which diseases one is predisposed to. However, jumping directly from A to C eliminates a large majority of people that did not follow the most common path, thus disenfranchising them from receiving accurate medical care. Eliminating social constructs from medical treatment and diagnosis is an endeavor that the entire field should embark on.
On the other hand, when it comes to recruiting participants for large scale observational studies, clinical trials, etc. whether or not social constructs such as gender and racial identity should be accounted for is an outstanding question. Using clinical trials as an example, ensuring that the proposed experimental treatment works well on all races and genders is of utmost importance and has often been overlooked in historical trials. However, would using lifestyle in order to recruit not serve the same purpose? And be more accurate? Would taking detailed history and lifestyle cause too much strain during recruitment and completely offset its advantages? Would statistics be too difficult to run on family history and lifestyle when we know it’s possible and established using gender and racial identity. I leave you with some food for thought.
This is a guest post by Antoine S. Johnson, Ph.D. Candidate, UCSF History of Health Sciences.
The 2020 police killings of Breonna Taylor and George Floyd facilitated important dialogue about racism being a public health issue. It also led to myriad student demands at college campuses throughout the nation, including at UCSF. Students demanded course curriculum addressing racism in science and medicine, with the hopes that such information and classes would be integrated in their field. One of the results were Grad 202: Racism in Science, which was taught in the Fall 2020 quarter by Dr. Aimee Medeiros and me. Almost 200 students enrolled in the course, causing us to create two sections. As a Ph.D. candidate in UCSF’s History of Health Sciences program, this was an invaluable experience that allowed me to build community with several students in the class who are now working on an article on the importance of such classes in science programs.
Demand remained high after the class, culminating in mini courses, including this one, that would continue such conversations and answer student requests. Grad 219: The Black Experience in American Medicine, examines ways Black people have not only been the victims of medical racism, but also how they contributed to the creation and expansion of medicine and science; how they have operated in their respected fields; and the harm caused by biological deterministic arguments of so-called racial differences. Although only three weeks long, students will leave this class with an understanding of the medical community’s relationship with African Americans from the antebellum period to the present. From an analytical perspective, this class will foster honest and open conversations about the assigned material. Additionally, students will have the opportunity to share their thoughts on any conversation, reading, video, or observation through weekly blog posts that will be published here, on the UCSF Archives & Special Collection, Brought to Light blog. These are not polished submissions but are rather their takeaways on things that stood out to them. In doing so, they will be able to offer one another constructive feedback by commenting on each other’s posts to continue pertinent conversations.
Thank you, and welcome to Grad 219 Course: The Black Experience in American Medicine.
Founding members at the UCSF Black Caucus Gala in February 2005. From the left to right: Elba Clemente-Lambert, Charles Clarey, Claudette Coleman, Freeman Bradley, Anitra (Koehler) Patterson, Paul Porter, Leon Johnson, and Walter “Pop” Nelson (sitting).
We are thrilled to announce that the UCSF Black Caucus Records digital collection has added and updated descriptions for over 400 items. The collection documents the history of the UCSF Black Caucus, which began in 1968 to address the social inequalities and inequities at the University of California. It contains photographs, videos, correspondence, publications, and meeting materials about the formation and activities of the Black Caucus. Some of the major events held by the UCSF Black Caucus include the protest to end of racism and discrimination at the University of California, the Dr. Martin Luther King, Jr. Week and Black History Month programs, in conjunction with other campus organizations including the Women’s Resource Center, and annual Gala fundraisers.
Founding members of the UCSF Black Caucus in December 2013 at the Millberry Union following Dr. Daniel Lowenstein’s “Last Lecture Series” at Cole Hall. . Standing, left to right, are Bill Stevens, Joseph Lambert, Elba Clemente-Lambert, Michael Adams, Norma Faris Taylor, Dr. John Watson, and Charles Clarey. Sitting, left to right, are Joanne Lewis, Carol Yates, Ethel Adams, Crystal Morris, Karen Newhouse.
A substantial portion of this incredible collection was complied, preserved, and donated to the archives by Elba Clemente-Lambert. Throughout the recent metadata enrichment project, she has painstakingly researched and provided more detailed descriptions of events and identification of individuals in photographs. Mrs. Clemente-Lambert collaborated with her UCSF colleagues and former Black Caucus members (now retirees) on what became a true crowdsourcing project that couldn’t have been successfully accomplished without her guidance and community support. (We will list the names of all people who supported this project in future blog posts). These additions will enable users to learn about the organization’s history, membership, leadership, and accomplishments.
Elba Clemente-Lambert
Elba Clemente-Lambert was born and raised in Spanish Harlem in the Upper East Side of Manhattan, New York. Mrs. Clemente-Lambert received her bachelor’s degree in Business Administration with a minor in Psychology from the City University of New York. She began her career in 1968 at UCSF as a Secretary II in the Department of Neurology. Then, she obtained an on-the-job training position (initiated by the efforts of the UCSF Black Caucus) in the Personnel Department (now Human Resources). Soon after joining the University of California, Elba became one of the founding members of the UCSF Black Caucus. She was elected to various positions in the Black Caucus’ Steering Committee, including Corresponding Secretary and Chair of the Publications Committee, as well as Member-at-Large. However, one of her most important positions was as “the unofficial, but official” photographer. Her passion for photography began in her high school journalism class, which stirred her belief that “we need to document what is occurring in our environment and beyond”. This dedication unintentionally led her to become a historian for the UCSF Black Caucus. Elba worked at UCSF until 1997 when she retired as a Senior Human Resource Specialist. In retirement, Elba continued to work occasionally with the UCSF Black Caucus while involved in the management of Creative Music Emporium (records store), established in April 1985 together with her late husband, first Black Officer hired at UCSF, Joseph G. Lambert, who decided to change his career after serving 18 years to become an entrepreneur in the music industry.
We would like to express our gratitude to all those who helped make this project possible: Mrs. Clemente-Lambert, Marisa McFarlane, and Charles Macquarie.
To learn more about the current activities of the UCSF Black Caucus, check out this link: https://blackcaucus.ucsf.edu/
To explore more materials from the UCSF Black Caucus Records, check out the collection on digital portal, Calisphere and the Online Archive of California (OAC).
UCSF Archives & Special
Collections was awarded a $14,986 local assistance grant by the California
State Library for the “Documenting the LGBTQ Health Equity Movement in
California” project.
Preserving
California’s LGBTQ History
is a grant program that funds projects that support physical and/or digital
preservation and digitization of lesbian, gay, bisexual, transgender, and queer
(LGBTQ) materials relating to California history and culture. This California
State Library program will award a total of $500,000 in one-time grants for
projects from large archival institutions with a global reach, as well as
smaller, localized collections. The program aims to preserve materials that
demonstrate the significant role of LGBTQ Californians and the LGBTQ movement
in this state, as well as providing a more comprehensive and inclusive view of
California’s history.
The UCSF project will support
preservation through processing and partial digitization of two collections
documenting the LGBTQ health equity movement in California:
• San Francisco AIDS Foundation Magnet Program Records
• UCSF LGBT Resource Center Records
San Francisco AIDS Foundation Magnet Program card
The San Francisco AIDS
Foundation (SFAF) Magnet Program is a health and wellness program located in
the SFAF’s Strut Center in the heart of the Castro District of San Francisco.
They offer community events, sexual health services, substance use counseling,
PrEP, HIV and STI testing, learning events and rotating art displays from queer
artists. In spring 2001, a Community
Advisory Board comprised of community members, social workers, and activists
began meeting regularly to discuss how to proceed with the development of a new
Gay Men’s Health Center. The new center chose
to address gay men’s health in innovative ways instead of simply replicating
existing programs in a new location. Since 2003, Magnet’s overarching vision
has been to promote the physical, mental, and social well-being of gay men.
Magnet activities are guided by the following core values of the agency:
self-determination, access, sexual expression, diversity, and leadership.
Magnet provides individual STI/HIV services and community programs including
book readings, art exhibits, town hall forums, and other social events. In 2007
Magnet merged with the SFAF to increase the services available to men
throughout the Bay Area. Magnet also serves transgender, gender non-conforming,
gender non-binary, and gender-queer people.
This collection includes
founding documents, surveys of clients, assessments of services, marketing
materials, advocacy campaigns, photographs, community art pieces, and posters
documenting the establishment and activities of the Magnet program.
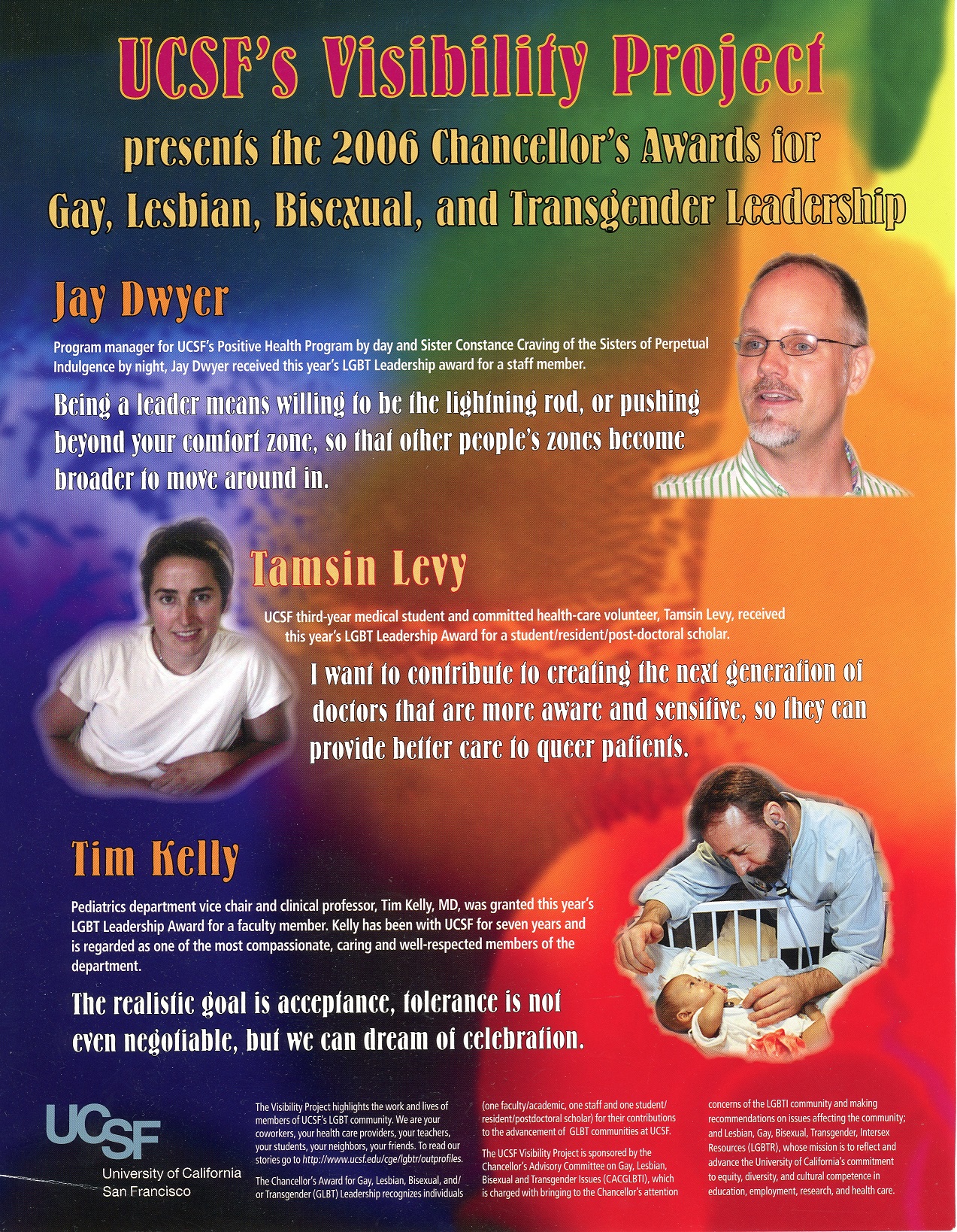
UCSF Visibility Project flyer, 2006 Chancellor’s Award for Gay, Lesbian, Bisexual, and Transgender Leadership
The LGBT Resource Center
serves as the hub for all queer life at UCSF, including the campus and medical
center. It works toward creating and maintaining a safe, inclusive, and
equitable environment for LGBTQIA+ students, staff, faculty, post-docs,
residents, fellows, alumni, and patients. It aims to sustain visibility and a
sense of community throughout the many campus sites. This community takes an
intersectional approach and is committed to building workplace equity,
promoting student and staff leadership, and providing high-quality,
culturally-congruent care to UCSF patients. Founded in 1998, it was the first
LGBT resource center in a health science institution.
This collection includes the center’s
founding documents, traces the earlier LGBT community activities in the 1970s
through the 1980s, and contains materials chronicling the history and evolution
of the center. It also includes records of diverse events organized by the
center: Coming Out Monologues, Trans Day of Remembrance & Resilience, and
Trans Day of Visibility, as well as correspondence and announcements related to
OUTlist, Mentoring Program, and Annual LGBTQIA+ Health Forum. These materials also
document UC-wide advocacy work for providing equal benefits for same-sex
domestic partners.
The UCSF Archives & Special
Collections have been working on preserving materials documenting the LGBTQ
health equity movement in California. These two recently acquired collections
will enable researchers to investigate these communities’ efforts to address health-related
issues and advocate for health equity.
The Magnet collections allow researchers to
investigate how the “San Francisco model” of AIDS care continued to evolve in
the twenty-first century by providing free and equitable health care, education,
and community space. Both collections contribute to an understanding of the
medical, social, and political processes that merged to develop effective means
of treating those with AIDS and other illnesses.
Diverse audiences will benefit
from having access to this project’s archival collections, including scholars
in disciplines such as medicine, nursing, jurisprudence, journalism, history
and sociology, college students, and members of the general public pursuing
individual areas of interest.
The collections included in
this project are currently only accessible at the UCSF Archives reading room.
The digitization of these collections will grant access to these valuable
primary sources and other hard-to-find materials to scholars, students, and
others worldwide. This project will significantly expand the historical record
of the LGBTQ health equity movement in California and make a new corpus of
materials related to the movement’s progress discoverable to a broad audience.
Over the past three decades, UCSF Archives & Special Collections has played a vital role in documenting the AIDS epidemic.
We are seeking your help to maintain and grow the AIDS History Project (AHP) archive as a critical, one-of-a-kind public record of the institutions and individuals involved in containing and treating the HIV both locally, and worldwide.
Please help support the UCSF AIDS History Project. We are hoping you will donate today and help us raise $50,000 by 2/1/2020 –please take a moment to do it now.
Your generosity advances vital work to collect, preserve, and provide universal access to stories of the AIDS epidemic.
35 years have passed since the beginning of the AIDS epidemic, and many of the original researchers, health care providers, and community activists who were on the front lines of defense against HIV have now begun to retire from public service. There is an urgent need to collect, preserve, and provide open access to their collections.
Your support will allow us to:
Catalog and digitize recently acquired collections, including, papers of Drs. Jay Levy and Steven G. Deeks, SF AIDS Foundation records
Record a new set of oral histories with clinicians, researchers, pharmaceutical and biotech scientists, health care workers, activists, community members, patients, and their family members
Expand the AIDS History Project statewide scope, solicit and acquire material fro regional community health centers
Organize exhibits and public events to share materials and stories preserved in the archives