In his recent article Dr. Brian Dolan looks at the politics of protests during the 1918 influenza epidemic in San Francisco.
“On April 17, 2020, San Francisco Mayor London Breed did something that had not been done for 101 years. She issued an order that face masks be worn in public as a measure to help prevent the spread of infectious disease in the midst of a pandemic. This act promptly raised questions about how things were handled a century ago. The media soon picked up on the antics of an “Anti-Mask League” that was formed in San Francisco to protest this inconvenience, noting some historical parallels with current public complaints about government overreach. This essay dives deeper into the historical context of the anti-mask league to uncover more information about the identity and possible motivations of those who organized these protests. In particular it shines light on the fascinating presence of the leading woman in the campaign—lawyer, suffragette, and civil rights activist, Mrs. E.C. Harrington.” Read the full story in Perspectives in Medical Humanities (UC Medical Humanities Consortium, May 19, 2020)
This is a guest post by Aaron J. Jackson, M.A, Ph.D. Candidate, UCSF History of Health Sciences.
From time to time, events in the
present so closely resemble events from the past that the aphorism “history
repeats itself” seems feasible. This can be demonstrated by comparing the
current crisis of the novel coronavirus with the influenza pandemic of 1918-1919.
The similarities are compelling. Like the SARS-CoV-2 coronavirus, the variety
of H1N1 influenza that swept across the world in 1918 and 1919 produced a
significant shock. It spread like wildfire, was frustratingly resistant to
contemporary therapeutics, exhibited novel characteristics, and forced
governments to resort to what some considered to be heavy-handed public health
interventions. Bay Area residents in 1918 were required to wear masks and
practice social distancing, just as they are required to do so today. Such
historical similarities are not, however, proof that history repeats itself.
But they do provide interesting opportunities for comparison between the past
and the present—opportunities that hold the potential to make the past more relatable
by building connections through common circumstances. And perhaps, through that
understanding, an opportunity for hope to shine in dark times.
This post is not an exhaustive
study comparing 1918 and 2020. Rather, it focuses on responses to crises and
specifically the ways that communities innovatively addressed shortages of
personal protective equipment (PPE). So, of course, it will be about war,
pandemics, socks, and sheet protectors. Naturally.
When the United States declared
war on the Imperial Government of Germany in April 1917, the nation was
woefully unprepared for the conflict. The war represented an unprecedented
crisis—one that required the federal government to assume new powers in order
to coordinate the resources of the entire nation. President Woodrow Wilson’s
administration worked with Congress to institute a draft to raise an army,
enacted strict economic control measures to conserve and direct resources
towards the production of war materiel, and passed laws that infringed on civil
liberties, all in the name of the war effort. To ensure public support for
these moves, the government mounted a massive propaganda campaign that appealed
to a specific version of American patriotism, appealing to citizens’ sense of
duty.
Mustering an army of sufficient size presented significant challenges. The men not only had to be inducted into military service—either by volunteering or being drafted—they required hundreds of training camps, transportation to those camps, equipment to train with, uniforms to wear. Once at the camps, they required food, shelter, and medical support. Military training was and remains a dangerous business, but the most significant medical problem at the cantonments was disease.
Base Hospital No. 30 “Officers and Enlisted Personnel” from the Woolsey (John Homer) Papers, MSS 70-5, UCSF Archives and Special Collections
As tens of thousands of American
recruits assembled at Army camps across the United States, they unwittingly
brought diseases with them, which found ample opportunity to spread in cramped
camp conditions. Most of these infections fell into the category of “common
respiratory unknown disease”—an unofficial designation among military recruits
who learned to add C.R.U.D. to the lexicon of military acronyms they learned.
The crud largely consisted of the common cold and other respiratory infections,
but cases of measles, mumps, and chicken pox were also common. Most cases of
the crud cleared up without need for treatment, but the prevalence of these
infections and the fact that new waves of infections would spring up with every
new trainload of recruits had the effect of masking a more dangerous threat.
Army physicians first identified more than 100 soldiers who had developed a
rather severe flu-like illness in March 1918. Within a week, the number of flu
cases at Fort Riley was over 500 and climbing. The H1N1 virus that caused the
influenza pandemic of 1918-1919 had arrived, but the nation was focused on the
war. And as American troops began arriving in France and moving into the front
lines—many of them no doubt bringing the virus with them—medical personnel
tasked with supporting the war effort shifted their focus from induction
screening and camp illnesses to other health concerns.
The First World War introduced a bevy of new ways to mangle and maim human bodies. From high-velocity rifle rounds and machine guns to high-explosive artillery shells, flamethrowers, hand grenades, aerial bombardment, and chemical weapons, the U.S. Army Medical Corps understood that the hospital system it established in France had to be prepared first and foremost for trauma care, which posed significant challenges. Not only did modern weapons cause extensive damage, the risks of sepsis and gangrene in an era before the discovery of antibiotics were high. Complicating this, European battlefields tended to stretch across agricultural land, teeming with bacteria after years of fertilization. Soldiers wounded on the front lines thus ran an extremely high risk of bacterial infection. To address this, the Medical Corps and its affiliates prioritized training Army health care workers in antiseptic wound care.
“U.S. Army Base Hospital No. 30, World War I (University of California School of Medicine Unit),” from The Thirtieth, AR 207-16, UCSF Archives and Special Collections
The experiences of the personnel of Base Hospital No. 30 are instructive in this regard. Base Hospital Thirty was the military hospital unit assembled from physicians, surgeons, and nurses associated with the University of California’s School of Medicine—the precursor to UCSF. Organized with the help of the American Red Cross Society shortly after Congress declared war, the unit spent more than a year training for the anticipated challenges of running a hospital for wounded soldiers in France. The unit’s nurses received orders to depart San Francisco on December 26, 1917 and reported to Army cantonment camps along the East Coast to help care for soldiers who had fallen ill with the crud, gaining invaluable experience in nursing soldiers and recognizing disease presentation. The unit’s surgeons practiced the ancient technique of wound debridement—removing foreign objects and cutting away dead and dying flesh to produce a clean wound—and attended clinical instruction that prepared them for the types of injuries they would face. And the unit’s corpsmen trained in the production and use of the Carrell-Dakin solution, a novel antiseptic more effective than carbolic acid and iodine but also a solution that required careful training and preparation. Thanks to training like this, the base hospital system was able to treat more than 300,000 sick and wounded soldiers with remarkably low mortality rates compared to previous wars.
Indeed, the medical apparatus and personnel organized to support the American Expeditionary Forces were well prepared for the anticipated hazards of the war. But in one of the remarkable parallels to the current coronavirus crisis, their job was perhaps made more difficult by the failure of American logistics in providing adequate personal protective equipment. But the shortage in 1918 was not one of N95 masks; rather, it was a matter of needing socks.
Today, the Occupational Safety
and Health Administration defines PPE as “equipment worn to minimize exposure
to hazards that cause serious workplace injuries and illnesses.”[i]
Under this definition, and in the context of soldiering, a good pair of socks
certainly applies. Trench warfare was a dirty business. It also tended to be
cold and wet—the perfect climate for a condition known today as “trench foot.”
Afflicted soldiers’ feet would go numb, swell, develop sore and infections, and
in extreme cases become gangrenous, possibly requiring amputation. Obviously,
this ran the risk of keeping soldiers from the front lines and thus undermining
the war effort. But ensuring a plentiful supply of clean dry socks somehow
slipped through the cracks of the Army’s logistical efforts to prepare for the
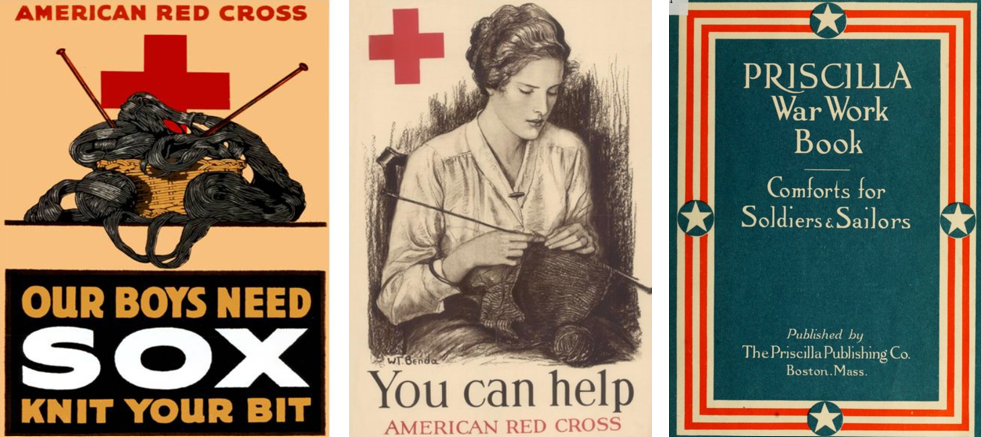
war. Fortunately, the American Red Cross and thousands of civilian volunteers
found ways to meet the challenge.
Beginning in 1917, the Red Cross put out calls for knitted garments, especially socks. The organization distributed officially-endorsed knitting patterns and free wool to anyone willing to “knit your bit.” The Priscilla War Work Book contains roughly a dozen such patterns ranging from socks to coats and winter hats.[ii] But the demand was greatest for socks. Across the country, knitters worked individually at home and collectively in social groups to try to keep up with the demand. Those who could not knit were urged to purchase or donate wool for the cause. Some organizations turned to mechanical solutions. The Seattle Red Cross utilized a knitting machine to produce long wool tubes that could be cut into 27-inch lengths, requiring only the toes to be stitched by hand.[iii] In this way, those behind the front lines were able to support the war effort by providing the PPE the soldiers needed to keep themselves in fighting shape.
Celebrating the end of the First World War in San Francisco, November 11, 1918. Image from The San Francisco Chronicle files.
Celebrating the end
of the First World War in San Francisco, November 11, 1918. Image from The San Francisco Chronicle files.
The knitting campaign continued
until the war ended with the declaration of the armistice on November 11, 1918.
By then, the nation was in the midst of the first wave of the influenza
pandemic. On October 9, 1918, San Francisco’s hospitals reported 169 influenza
cases. A week later, there were more than 2,000 and the city’s Board of Health
issued recommendations for social distancing.[iv]
With so many health care professionals supporting the war effort, the Bay
Area’s medical infrastructure was stretched to the limit and cities put out
calls for volunteers. Hospital space soon became a valuable commodity and many
facilities, including the Oakland Municipal Auditorium, were converted into
temporary hospitals, and public health officials began recommending the use of
face masks, which they later made mandatory.[v]
But it is important to remember that these were local efforts to respond to the
pandemic. The federal government, which had mustered the resources of the
entire nation to fight the war in Europe, was unwilling to do the same to
combat the pandemic at home, leaving it up to local authorities, medical
institutions, and volunteer organizations to make do as best they could.
“Oakland Municipal Auditorium is used as a temporary hospital,” 1918, Oakland Public Library
Unfortunately, we find ourselves
in a similar situation today. As the novel coronavirus took on pandemic
proportions, stores of PPE for frontline healthcare workers reached critical
levels. Before the pandemic, China produced approximately half the world’s
supply of medical masks. As the infection spread in China, their exports
stopped, and the resulting shortage spurred competition between institutions
and governments to secure PPE, which only exacerbated the situation.
Thankfully, a multidisciplinary team at UCSF found a way to be a part of the
solution, echoing the efforts of American knitters from over a century ago.
From left to right: UCSF shield frames,; A completely assembled UCSF face shield; Dr. Alexis Dang wears an assembled face shield over a N-95 respirator. For additional information please read the UCSF Library Makers Lab story. UCSF Library Makers Lab Left to right: UCSF shield frames,; A completely assembled UCSF face shield; Dr. Alexis Dang wears an assembled face shield over a N-95 respirator. For additional information please read the UCSF Library Makers Lab story
Noting the need for face shields, experts at UCSF specializing in biochemistry, engineering, logistics, medical workplace safety, and 3D model design came together in March 2020 to develop something that could help address the PPE shortage. By April, the team completed designs for three different models of 3D-printable face shield frames that, when combined with rubber bands and transparent document protectors, serve as functional and reusable face shields. They then collected seventeen 3D printers from across the university and turned the UCSF Makers Lab in the Kalmanovitz Library into an ad hoc face shield factory that can produce more than 300 shields each day—enough to supply UCSF’s front-line health care workers and then some.[vi] Extra shields are distributed to Bay Area hospitals. Moreover, like the Red Cross with the distribution of the Priscilla War Work Book, the UCSF team is sharing their plans in an open source repository so that others can emulate their efforts.[vii] This allows those with access to 3D printers and a few dollars’ worth of office supplies to contribute to the ongoing PPE shortage by producing face shields that have been designed, tested, and vetted by experts at one of the nation’s leading medical institutions.
Certainly, there are remarkable
similarities to be drawn between the modern crisis and those in the past. Once
again, the government was unprepared for a crisis despite advanced warning.
Once again, people are working in the front lines to save others despite
inadequate supplies. And once again, like the First World War and the influenza
pandemic of 1918-1919, the coronavirus pandemic is a devastating event likely
to be measured in the tally of lives lost. In the face of such grim statistics,
it is easy to fall into cynicism and say that history is repeating.
In 1905, philosopher George
Santayana explored the notion of progress—the idea that things move toward
improvement—and stated that “those who cannot remember the past are condemned
to repeat it.”[viii]
This is likely the origin of the aphorism “history repeats itself.” But Santaya
was not making a hopeless argument; rather, he noted that if progress is to be achieved,
it will be because humans not only record the past, they engage with it, learn
from it, and seek to understand it. And how that is achieved depends on the
ability to draw relatable connections with the past that emphasize human
agency. In 1918, knitters took up their needles. Today, a team of scientists,
engineers, and others figured out how to make face shields using 3D printers
and office supplies. These may seem like small contributions in the grand
scheme of things, but they are important examples of positive human agency in
the face of crisis.
[ii]
Elsa
Schappel Barsaloux and the American National Red Cross, The Priscilla War
Work Book: Including Directions for Knitted Garments and Comfort Kits from the
American Red Cross, and Knitted Garments for the Boy Scout. Boston, Mass.:
The Priscilla Publishing Company, 1917. Available at the HathiTrust Digital
Library. https://hdl.handle.net/2027/loc.ark:/13960/t2988wd21
[iv]
“Thirty-Seven New Cases Found in S.F.,” San Francisco Chronicle 10 Oct.
1918, 3; “Hassler Urges Churches and Theaters to Close,” San Francisco
Chronicle 17 Oct. 1918, 5.
[v]
“Wear a Mask and Save Your Life!” San Francisco Chronicle, 22 Oct. 1918.
By Erin Hurley, User Services & Accessioning Archivist
Although, in 2020, advice like “wash your hands” and “cover
your mouth when you cough” seem fairly obvious and common sense, there was a
time when this was not the case. That time was March 1855, when the situation
in British hospitals outside of Constantinople (now Istanbul, Turkey) during
the Crimean War had become so dire that Florence Nightingale and 40 other women
acting as trained volunteer nurses were finally allowed access to patients
(they had previously been denied access because of their gender). Hospitals
were overcrowded and extremely unsanitary conditions encouraged the spread of
infectious diseases like cholera, typhoid, typhus and dysentery, which Nightingale
recognized immediately. She implemented basic cleanliness measures, such as
baths for patients, clean facilities, and fresh linens, and advocated for an
approach that addressed the psychological and emotional, as well as the
physical, needs of patients. Her improvements brought a dramatic decline in the
mortality rate at these hospitals, which had previously been as high as 40%.
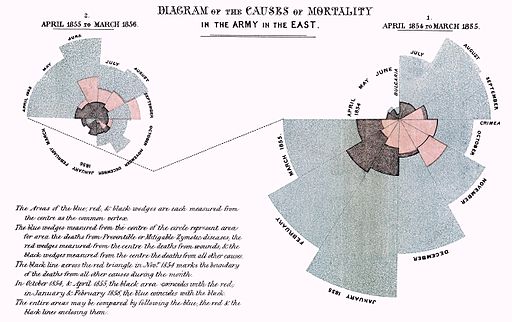
While Nightingale is well known as one of the world’s first nurses, she is less well known for her strikingly lovely data visualizations (including pie charts and a rose-shaped design called the “coxcomb”), which she used to highlight the number of deaths from diseases, in addition to deaths from wounds or injury, during the Crimean War. Nightingale, a mathematician and statistician, recognized the importance of eye-catching visuals in communicating the impact of her innovations.
w:Florence Nightingale (1820–1910). / Public domain, courtesy of Wikimedia Commons
National Nurses Week begins each year on May 6th (National Nurses Day) and ends each year on May 12th (Florence Nightingale’s birthday). Today, we celebrate the history of nursing and nurses of all kinds, and the essential, life-saving work that they perform. We hope you enjoy this series of digital images from UCSF’s Archives and Special Collections, all digitized and available online through Calisphere. Archives and Special Collections also holds the fascinating Florence Nightingale Memorial Collection, created by Country Joe McDonald of Country Joe & the Fish, which you can read more about here.
Nuns gathered around an iron lung, undated, from St. Joseph College of Nursing records, MSS 81-10 and MSS 94-35St. Joseph College of Nursing tree planting ceremony by Don Bosco Studios, S.F., circa 1940-1960, St. Joseph College of Nursing records, MSS 81-10 and MSS 94-35Nurses in the library, circa 1950s, UCSF Medical Center at Mount Zion ArchivesNursing students playing records and reading in dormitory, 1955, Photograph Collection, School of NursingFaculty instructor in Anatomy and Physiology Laboratory at St. Joseph College of Nursing by Ashworth of London, circa 1960, St. Joseph College of Nursing records, MSS 81-10 and MSS 94-35Moffitt Hospital floor nurse with IV drip by Dennis Galloway, 1969, Photograph Collection, School of NursingGladys W. Henderson, 1971, Photograph Collection, School of Nursing S/N, LVN Graduates and Training ProgramMoffitt Hospital nurses station by Richard Weymouth Brooks, circa 1984, from Photograph Collection, School of Nursing, Nursing ServicesMount Zion nursing assistant Michael Wollflair examines patient David Earl by David Powers, 1994, MSS 2009-15, Powers (David) Photograph CollectionLicensed Vocational Nurse (LVN) Training Program graduates, 1971, Photograph Collection, School of Nursing S/N, LVN Graduates and Training Program