This is a guest post by Antoine S. Johnson, Ph.D. Candidate, UCSF History of Health Sciences.
The 2020 police killings of Breonna Taylor and George Floyd facilitated important dialogue about racism being a public health issue. It also led to myriad student demands at college campuses throughout the nation, including at UCSF. Students demanded course curriculum addressing racism in science and medicine, with the hopes that such information and classes would be integrated in their field. One of the results were Grad 202: Racism in Science, which was taught in the Fall 2020 quarter by Dr. Aimee Medeiros and me. Almost 200 students enrolled in the course, causing us to create two sections. As a Ph.D. candidate in UCSF’s History of Health Sciences program, this was an invaluable experience that allowed me to build community with several students in the class who are now working on an article on the importance of such classes in science programs.
Demand remained high after the class, culminating in mini courses, including this one, that would continue such conversations and answer student requests. Grad 219: The Black Experience in American Medicine, examines ways Black people have not only been the victims of medical racism, but also how they contributed to the creation and expansion of medicine and science; how they have operated in their respected fields; and the harm caused by biological deterministic arguments of so-called racial differences. Although only three weeks long, students will leave this class with an understanding of the medical community’s relationship with African Americans from the antebellum period to the present. From an analytical perspective, this class will foster honest and open conversations about the assigned material. Additionally, students will have the opportunity to share their thoughts on any conversation, reading, video, or observation through weekly blog posts that will be published here, on the UCSF Archives & Special Collection, Brought to Light blog. These are not polished submissions but are rather their takeaways on things that stood out to them. In doing so, they will be able to offer one another constructive feedback by commenting on each other’s posts to continue pertinent conversations.
Thank you, and welcome to Grad 219 Course: The Black Experience in American Medicine.
This is a guest post by Aaron J. Jackson, M.A, Ph.D. Candidate, UCSF History of Health Sciences.
From time to time, events in the
present so closely resemble events from the past that the aphorism “history
repeats itself” seems feasible. This can be demonstrated by comparing the
current crisis of the novel coronavirus with the influenza pandemic of 1918-1919.
The similarities are compelling. Like the SARS-CoV-2 coronavirus, the variety
of H1N1 influenza that swept across the world in 1918 and 1919 produced a
significant shock. It spread like wildfire, was frustratingly resistant to
contemporary therapeutics, exhibited novel characteristics, and forced
governments to resort to what some considered to be heavy-handed public health
interventions. Bay Area residents in 1918 were required to wear masks and
practice social distancing, just as they are required to do so today. Such
historical similarities are not, however, proof that history repeats itself.
But they do provide interesting opportunities for comparison between the past
and the present—opportunities that hold the potential to make the past more relatable
by building connections through common circumstances. And perhaps, through that
understanding, an opportunity for hope to shine in dark times.
This post is not an exhaustive
study comparing 1918 and 2020. Rather, it focuses on responses to crises and
specifically the ways that communities innovatively addressed shortages of
personal protective equipment (PPE). So, of course, it will be about war,
pandemics, socks, and sheet protectors. Naturally.
When the United States declared
war on the Imperial Government of Germany in April 1917, the nation was
woefully unprepared for the conflict. The war represented an unprecedented
crisis—one that required the federal government to assume new powers in order
to coordinate the resources of the entire nation. President Woodrow Wilson’s
administration worked with Congress to institute a draft to raise an army,
enacted strict economic control measures to conserve and direct resources
towards the production of war materiel, and passed laws that infringed on civil
liberties, all in the name of the war effort. To ensure public support for
these moves, the government mounted a massive propaganda campaign that appealed
to a specific version of American patriotism, appealing to citizens’ sense of
duty.
Mustering an army of sufficient size presented significant challenges. The men not only had to be inducted into military service—either by volunteering or being drafted—they required hundreds of training camps, transportation to those camps, equipment to train with, uniforms to wear. Once at the camps, they required food, shelter, and medical support. Military training was and remains a dangerous business, but the most significant medical problem at the cantonments was disease.
Base Hospital No. 30 “Officers and Enlisted Personnel” from the Woolsey (John Homer) Papers, MSS 70-5, UCSF Archives and Special Collections
As tens of thousands of American
recruits assembled at Army camps across the United States, they unwittingly
brought diseases with them, which found ample opportunity to spread in cramped
camp conditions. Most of these infections fell into the category of “common
respiratory unknown disease”—an unofficial designation among military recruits
who learned to add C.R.U.D. to the lexicon of military acronyms they learned.
The crud largely consisted of the common cold and other respiratory infections,
but cases of measles, mumps, and chicken pox were also common. Most cases of
the crud cleared up without need for treatment, but the prevalence of these
infections and the fact that new waves of infections would spring up with every
new trainload of recruits had the effect of masking a more dangerous threat.
Army physicians first identified more than 100 soldiers who had developed a
rather severe flu-like illness in March 1918. Within a week, the number of flu
cases at Fort Riley was over 500 and climbing. The H1N1 virus that caused the
influenza pandemic of 1918-1919 had arrived, but the nation was focused on the
war. And as American troops began arriving in France and moving into the front
lines—many of them no doubt bringing the virus with them—medical personnel
tasked with supporting the war effort shifted their focus from induction
screening and camp illnesses to other health concerns.
The First World War introduced a bevy of new ways to mangle and maim human bodies. From high-velocity rifle rounds and machine guns to high-explosive artillery shells, flamethrowers, hand grenades, aerial bombardment, and chemical weapons, the U.S. Army Medical Corps understood that the hospital system it established in France had to be prepared first and foremost for trauma care, which posed significant challenges. Not only did modern weapons cause extensive damage, the risks of sepsis and gangrene in an era before the discovery of antibiotics were high. Complicating this, European battlefields tended to stretch across agricultural land, teeming with bacteria after years of fertilization. Soldiers wounded on the front lines thus ran an extremely high risk of bacterial infection. To address this, the Medical Corps and its affiliates prioritized training Army health care workers in antiseptic wound care.
“U.S. Army Base Hospital No. 30, World War I (University of California School of Medicine Unit),” from The Thirtieth, AR 207-16, UCSF Archives and Special Collections
The experiences of the personnel of Base Hospital No. 30 are instructive in this regard. Base Hospital Thirty was the military hospital unit assembled from physicians, surgeons, and nurses associated with the University of California’s School of Medicine—the precursor to UCSF. Organized with the help of the American Red Cross Society shortly after Congress declared war, the unit spent more than a year training for the anticipated challenges of running a hospital for wounded soldiers in France. The unit’s nurses received orders to depart San Francisco on December 26, 1917 and reported to Army cantonment camps along the East Coast to help care for soldiers who had fallen ill with the crud, gaining invaluable experience in nursing soldiers and recognizing disease presentation. The unit’s surgeons practiced the ancient technique of wound debridement—removing foreign objects and cutting away dead and dying flesh to produce a clean wound—and attended clinical instruction that prepared them for the types of injuries they would face. And the unit’s corpsmen trained in the production and use of the Carrell-Dakin solution, a novel antiseptic more effective than carbolic acid and iodine but also a solution that required careful training and preparation. Thanks to training like this, the base hospital system was able to treat more than 300,000 sick and wounded soldiers with remarkably low mortality rates compared to previous wars.
Indeed, the medical apparatus and personnel organized to support the American Expeditionary Forces were well prepared for the anticipated hazards of the war. But in one of the remarkable parallels to the current coronavirus crisis, their job was perhaps made more difficult by the failure of American logistics in providing adequate personal protective equipment. But the shortage in 1918 was not one of N95 masks; rather, it was a matter of needing socks.
Today, the Occupational Safety
and Health Administration defines PPE as “equipment worn to minimize exposure
to hazards that cause serious workplace injuries and illnesses.”[i]
Under this definition, and in the context of soldiering, a good pair of socks
certainly applies. Trench warfare was a dirty business. It also tended to be
cold and wet—the perfect climate for a condition known today as “trench foot.”
Afflicted soldiers’ feet would go numb, swell, develop sore and infections, and
in extreme cases become gangrenous, possibly requiring amputation. Obviously,
this ran the risk of keeping soldiers from the front lines and thus undermining
the war effort. But ensuring a plentiful supply of clean dry socks somehow
slipped through the cracks of the Army’s logistical efforts to prepare for the
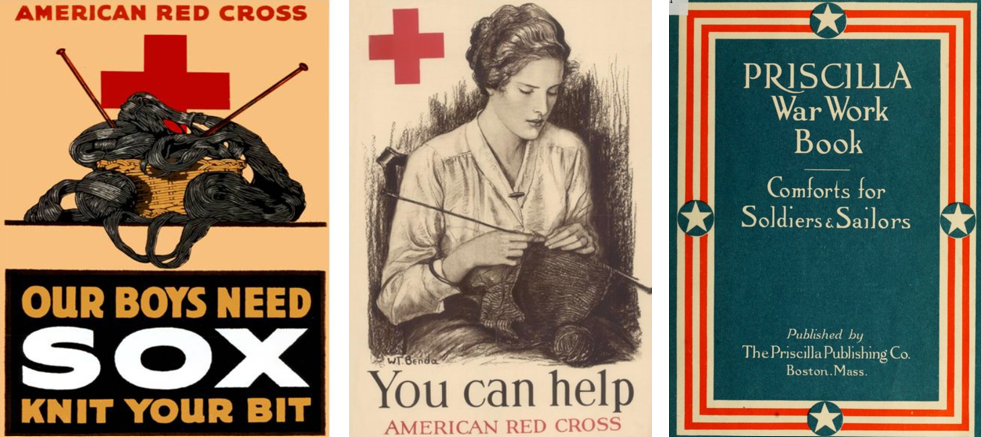
war. Fortunately, the American Red Cross and thousands of civilian volunteers
found ways to meet the challenge.
Beginning in 1917, the Red Cross put out calls for knitted garments, especially socks. The organization distributed officially-endorsed knitting patterns and free wool to anyone willing to “knit your bit.” The Priscilla War Work Book contains roughly a dozen such patterns ranging from socks to coats and winter hats.[ii] But the demand was greatest for socks. Across the country, knitters worked individually at home and collectively in social groups to try to keep up with the demand. Those who could not knit were urged to purchase or donate wool for the cause. Some organizations turned to mechanical solutions. The Seattle Red Cross utilized a knitting machine to produce long wool tubes that could be cut into 27-inch lengths, requiring only the toes to be stitched by hand.[iii] In this way, those behind the front lines were able to support the war effort by providing the PPE the soldiers needed to keep themselves in fighting shape.
Celebrating the end of the First World War in San Francisco, November 11, 1918. Image from The San Francisco Chronicle files.
Celebrating the end
of the First World War in San Francisco, November 11, 1918. Image from The San Francisco Chronicle files.
The knitting campaign continued
until the war ended with the declaration of the armistice on November 11, 1918.
By then, the nation was in the midst of the first wave of the influenza
pandemic. On October 9, 1918, San Francisco’s hospitals reported 169 influenza
cases. A week later, there were more than 2,000 and the city’s Board of Health
issued recommendations for social distancing.[iv]
With so many health care professionals supporting the war effort, the Bay
Area’s medical infrastructure was stretched to the limit and cities put out
calls for volunteers. Hospital space soon became a valuable commodity and many
facilities, including the Oakland Municipal Auditorium, were converted into
temporary hospitals, and public health officials began recommending the use of
face masks, which they later made mandatory.[v]
But it is important to remember that these were local efforts to respond to the
pandemic. The federal government, which had mustered the resources of the
entire nation to fight the war in Europe, was unwilling to do the same to
combat the pandemic at home, leaving it up to local authorities, medical
institutions, and volunteer organizations to make do as best they could.
“Oakland Municipal Auditorium is used as a temporary hospital,” 1918, Oakland Public Library
Unfortunately, we find ourselves
in a similar situation today. As the novel coronavirus took on pandemic
proportions, stores of PPE for frontline healthcare workers reached critical
levels. Before the pandemic, China produced approximately half the world’s
supply of medical masks. As the infection spread in China, their exports
stopped, and the resulting shortage spurred competition between institutions
and governments to secure PPE, which only exacerbated the situation.
Thankfully, a multidisciplinary team at UCSF found a way to be a part of the
solution, echoing the efforts of American knitters from over a century ago.
From left to right: UCSF shield frames,; A completely assembled UCSF face shield; Dr. Alexis Dang wears an assembled face shield over a N-95 respirator. For additional information please read the UCSF Library Makers Lab story. UCSF Library Makers Lab Left to right: UCSF shield frames,; A completely assembled UCSF face shield; Dr. Alexis Dang wears an assembled face shield over a N-95 respirator. For additional information please read the UCSF Library Makers Lab story
Noting the need for face shields, experts at UCSF specializing in biochemistry, engineering, logistics, medical workplace safety, and 3D model design came together in March 2020 to develop something that could help address the PPE shortage. By April, the team completed designs for three different models of 3D-printable face shield frames that, when combined with rubber bands and transparent document protectors, serve as functional and reusable face shields. They then collected seventeen 3D printers from across the university and turned the UCSF Makers Lab in the Kalmanovitz Library into an ad hoc face shield factory that can produce more than 300 shields each day—enough to supply UCSF’s front-line health care workers and then some.[vi] Extra shields are distributed to Bay Area hospitals. Moreover, like the Red Cross with the distribution of the Priscilla War Work Book, the UCSF team is sharing their plans in an open source repository so that others can emulate their efforts.[vii] This allows those with access to 3D printers and a few dollars’ worth of office supplies to contribute to the ongoing PPE shortage by producing face shields that have been designed, tested, and vetted by experts at one of the nation’s leading medical institutions.
Certainly, there are remarkable
similarities to be drawn between the modern crisis and those in the past. Once
again, the government was unprepared for a crisis despite advanced warning.
Once again, people are working in the front lines to save others despite
inadequate supplies. And once again, like the First World War and the influenza
pandemic of 1918-1919, the coronavirus pandemic is a devastating event likely
to be measured in the tally of lives lost. In the face of such grim statistics,
it is easy to fall into cynicism and say that history is repeating.
In 1905, philosopher George
Santayana explored the notion of progress—the idea that things move toward
improvement—and stated that “those who cannot remember the past are condemned
to repeat it.”[viii]
This is likely the origin of the aphorism “history repeats itself.” But Santaya
was not making a hopeless argument; rather, he noted that if progress is to be achieved,
it will be because humans not only record the past, they engage with it, learn
from it, and seek to understand it. And how that is achieved depends on the
ability to draw relatable connections with the past that emphasize human
agency. In 1918, knitters took up their needles. Today, a team of scientists,
engineers, and others figured out how to make face shields using 3D printers
and office supplies. These may seem like small contributions in the grand
scheme of things, but they are important examples of positive human agency in
the face of crisis.
[ii]
Elsa
Schappel Barsaloux and the American National Red Cross, The Priscilla War
Work Book: Including Directions for Knitted Garments and Comfort Kits from the
American Red Cross, and Knitted Garments for the Boy Scout. Boston, Mass.:
The Priscilla Publishing Company, 1917. Available at the HathiTrust Digital
Library. https://hdl.handle.net/2027/loc.ark:/13960/t2988wd21
[iv]
“Thirty-Seven New Cases Found in S.F.,” San Francisco Chronicle 10 Oct.
1918, 3; “Hassler Urges Churches and Theaters to Close,” San Francisco
Chronicle 17 Oct. 1918, 5.
[v]
“Wear a Mask and Save Your Life!” San Francisco Chronicle, 22 Oct. 1918.
In his talk at the UCSF Archives & Special Collections, Zach Bleemer will discuss how he has used data science – thousands of computer-processed versions of annual registers, directories, and catalogs – to reconstruct a near-complete database of all students, faculty, and courses at four-year universities in California in the first half of the 20th century, including UC San Francisco (which taught both undergraduates and graduate students at the time). Visualizations of this database display the expansion of higher education into rural California communities, the rise and fall of various academic departments and disciplines, and the slow (and still-incomplete) transition towards egalitarian major selection.
Zach will also discuss his recent CSHE Working Paper, in which he uses additional digitized records to analyze the social impact of the early 20th century’s expansion of female high school science teachers and female doctors across rural California communities. He finds that newly-arrived female STEM professionals serve as important role models for young women in these rural communities, causing substantial increases in female college-going. However, these young women are no more likely to study STEM fields or become doctors themselves.
Zach Bleemer
Zach Bleemer is a PhD student in Economics and Digital Humanities Fellow at UC Berkeley, where his research examines the educational and occupational decisions of young Americans. He has previously held senior research analyst positions at the Federal Reserve Bank of New York and Mathematica Policy Research, and has published working papers on student debt, parental coresidence, and university attendance. He is also currently a Research Associate at UC Berkeley’s Center for Studies in Higher Education and a Visiting Scholar at the Federal Reserve Bank of San Francisco.
UCSF Archives & Special Collections launched this lecture series to introduce a wider community to treasures and collections from its holdings, to provide an opportunity for researchers to discuss how they use this material, and to celebrate clinicians, scientists, and health care professionals who donated their papers to the archives.
Join UCSF Archives & Special Collections for an afternoon talk with medical historian and author Paul Blanc MD, MSPH, as he discusses the toxic legacy of viscose rayon portrayed in his new book, Fake Silk. Dr. Blanc poses a basic question: When a new technology makes people ill, how high does the body count have to be before protective steps are taken? His work tells a dark story of hazardous manufacturing, poisonous materials, environmental abuses, political machinations, and economics trumping safety concerns. It explores the century-long history of “fake silk,” or cellulose viscose, used to produce such products as rayon textiles and tires, cellophane, and everyday kitchen sponges. His research uncovers the grim history of a product that crippled and even served a death sentence to many industry workers while also releasing toxic carbon disulfide into the environment.
Viscose, an innovative and lucrative product first introduced in the early twentieth century, quickly became a multinational corporate enterprise. Blanc investigates industry practices from the beginning through two highly profitable world wars, the mid-century export of hazardous manufacturing to developing countries, and the current “green-washing” of viscose as an eco-friendly product. This work brings to light an industrial hazard whose egregious history ranks with those of asbestos, lead, and mercury.
Paul Blanc, MD, MSPH
Dr. Blanc holds the Endowed Chair in Occupational and Environmental Medicine at the UCSF, where he has been a faculty member since 1988. Blanc received his BA from Goddard College (Plainfield, Vermont), where he first became interested in health and the environment, later training at the Harvard School of Public Health (in industrial hygiene), the Albert Einstein School of Medicine, and Cook County Hospital (in a joint Occupational Medicine and Internal Medicine Residency). He was a Robert Wood Johnson Clinical Scholar at UCSF and later a Fulbright Senior Research Scholar at the Ben Gurion University of the Negev. He also has been a resident scholar at the Rockefeller Bellagio Center (Bellagio, Italy) and the American Academy in Rome. In 2013-4, he was a fellow at the Center for Advanced Studies in the Behavioral Sciences at Stanford University. Blanc is the author of How Everyday Products Make People Sick (University of California Press, 2009) also writes a blog, “Household Hazards,” that is hosted by the magazine Psychology Today. Fake Silk: The Lethal History of Viscose Rayon is published by Yale University Press.
UCSF Archives & Special Collections launched this lecture series to introduce a wider community to treasures and collections from its holdings, to provide an opportunity for researchers to discuss how they use this material, and to celebrate clinicians, scientists, and health care professionals who donated their papers to the archives.
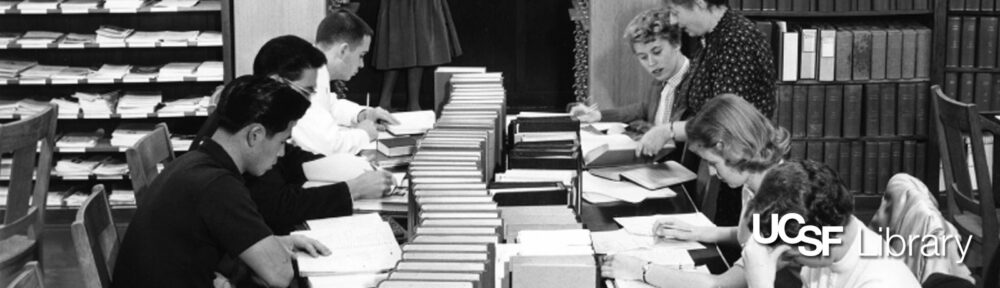
In observance of this lovely celebratory week, we bring you a few images of UCSF Library staff and librarians in their natural habitat from the 1950s.
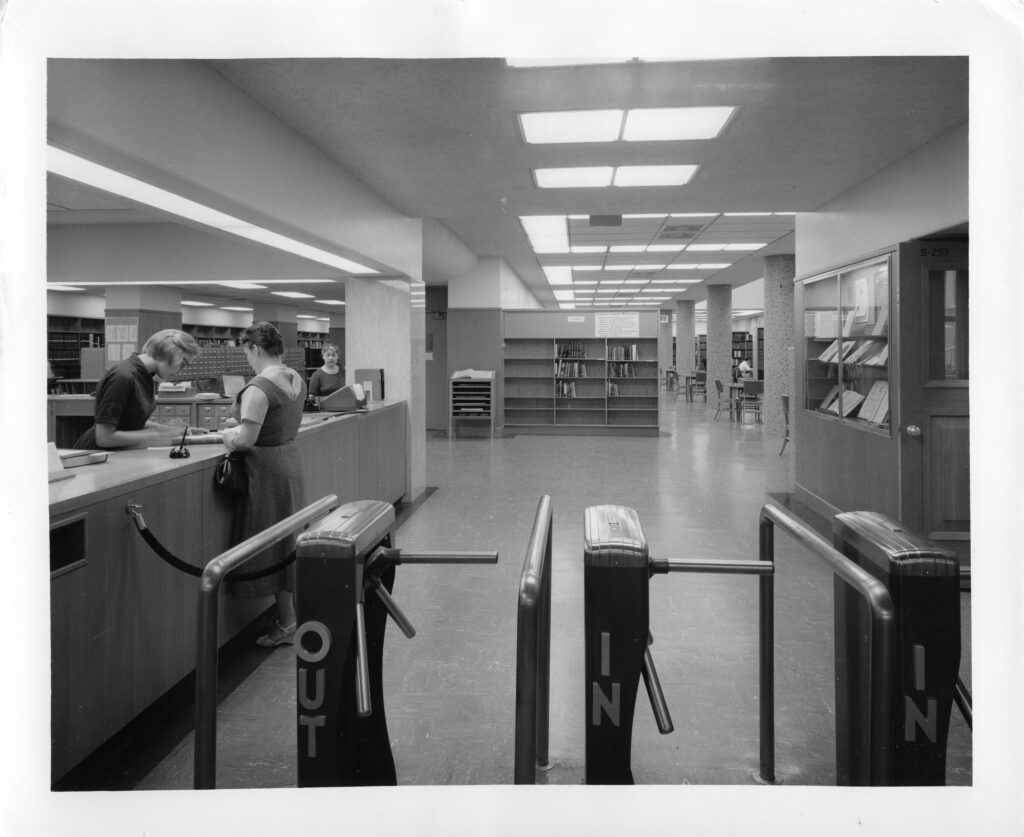
Photograph collection, Medical Sciences Building – The Library
Above, the entrance way to the old UCSF Library, in the Medical Sciences building, in 1959. Check out our previous post that expands a bit on the history of that library.
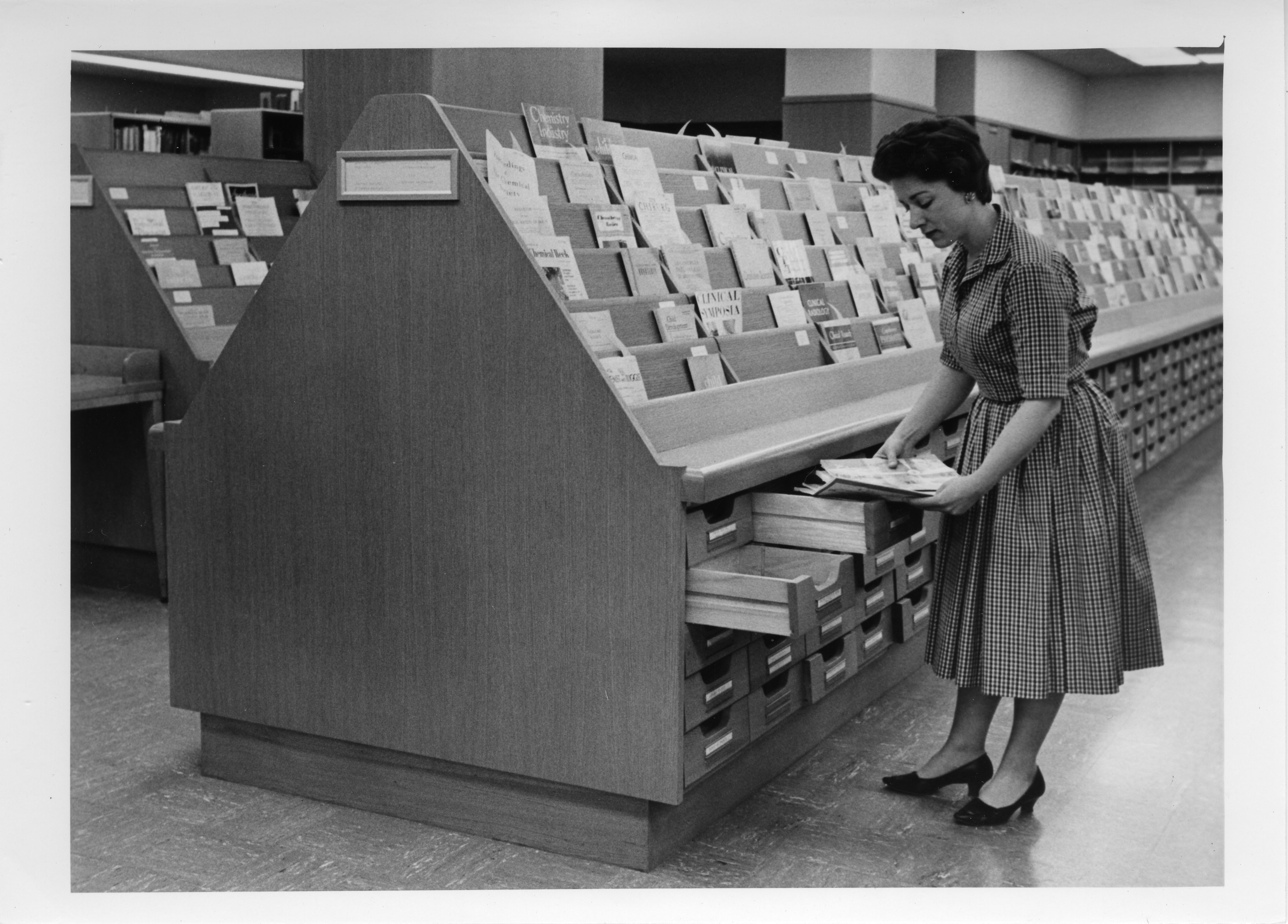
Photograph collection, Medical Sciences Building – The Library
Tidying the current periodicals section in the 1950s.
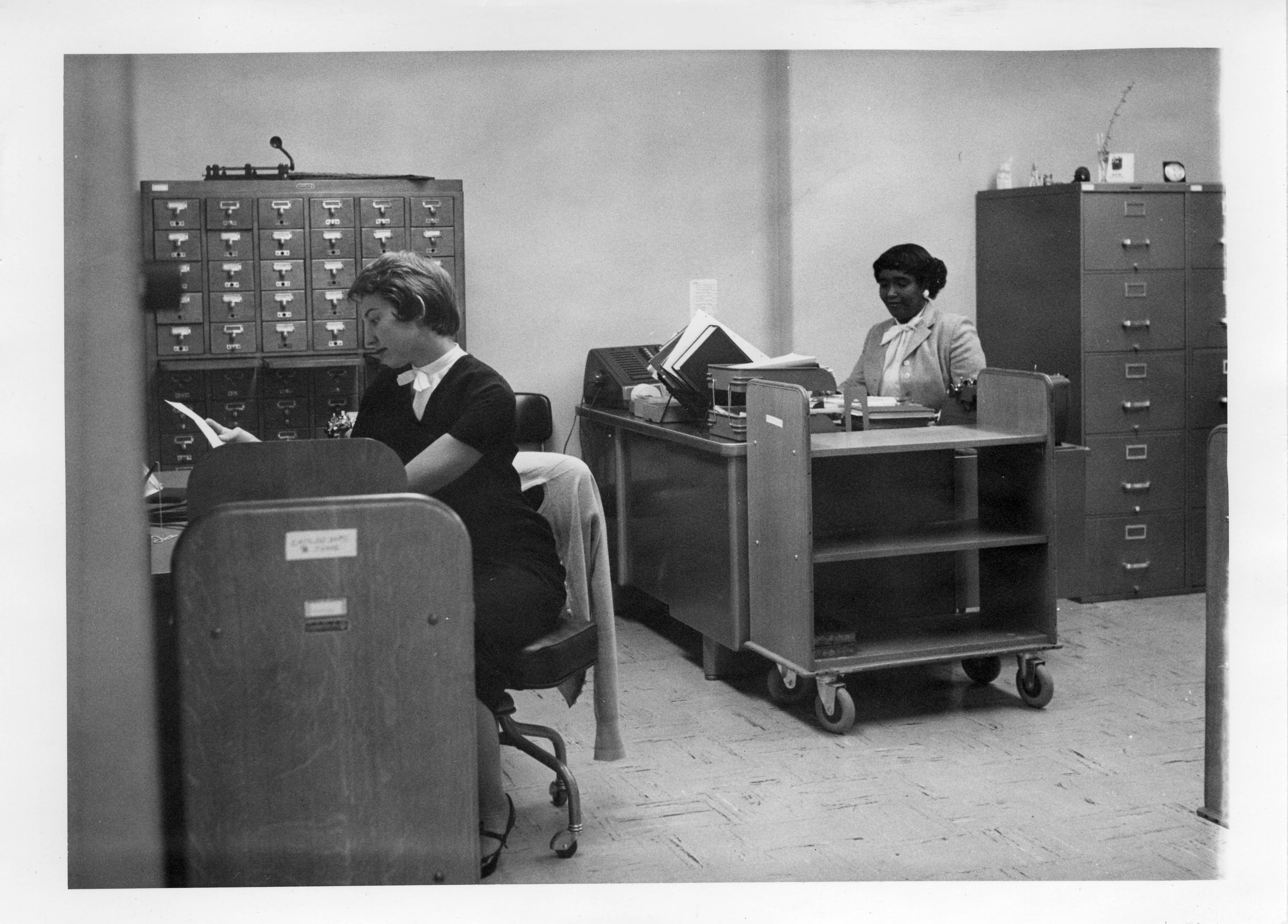
Photograph collection, Medical Sciences Building – The Library
Librarians of the Catalog Department (note card catalogs in the background) in the fall of 1958.
In honor of Women’s History Month, we’re spotlighting a few of the many talented and trailblazing women who have been important in the history of UCSF and you may not have heard of before.
Today, read a little about the remarkable life and career of Ellen Brown, MD. We are fortunate to have Brown’s manuscript collection, MSS 87-42, and her oral history in the UCSF Archives & Special Collections.
Ellen Brown was born in San Francisco in 1912. She and her older brother Fred were raised by her parents, Warner and Jessie Brown, in Berkeley. Jessie was a high school teacher and botanist and Warner was a professor of psychology at UC Berkeley. Fred died at the age of 16 of respiratory complications of polio. His death had a lasting impact on Brown– she dreamed of becoming a doctor as a child.
Ed Fong, Tesauro, and Brown in June, 1939.
Brown attended University High School in Oakland and went on to study at the University of California Berkeley, graduating with a bachelors degree in 1934. She continued to the UC Medical School’s San Francisco campus and graduated with her medical degree in 1939. In a class of 63 students, she was one of a handful of women.
Following graduation, Brown became chief resident under William J. Kerr, UC Chair of Medicine, from 1939-1943. The two worked closely for years– prioritizing cardiovascular research at UCSF. Brown helped to found the , which opened in 1958. Kerr was instrumental in laying the groundwork for the Cardiovascular Research Institute (CVRI), procuring the space on the 13th floor of Moffitt Hospital and funding from both UCSF and the National Heart Institute. The CVRI opened in 1958 with Brown as a co-founder and, later, a senior staff member. (Check out some of the CVRI’s milestones here.)
Ellen Brown at Harvard Medical School, 1946
Brown’s academic appointment at UCSF began with clinical instructor, 1943-1944, moved to associate professor, 1946-1959, and became professor of medicine in 1959. In 1944-1946 she was a Commonwealth Fund fellow in the Department of Physiology at Harvard Medical School (see photo above) and in 1958 she was a Guggenheim Fellow at Oxford University.
Brown operated a lab on campus for peripheral vascular research though the 1960s and 1970s. Concurrently, she worked on improving teaching techniques in predoctoral medical classes, initiating the “Introduction to Clinical Medicine” course and later serving as a residency evaluator for the School of Medicine.
This quote, from Brown’s oral history, demonstrates her zeal for education, enthusiasm for change in curriculum, and sense of humor: “The wonderful thing was how interested all these people in the non-medicine departments were. An ophthalmologist would sit down with a bunch of absolute nerds, and come and do that, four or five times, and teach them. The hardest thing to learn to do is to see in an ophthalmoscope. It is for most doctors. It’s one of the last things you feel comfortable about. That and a pelvic exam, I guess.”
Over the course of her illustrious career, Brown’s research interests included capillary pressure and permeability, blood volume and vascular capacity, cardiac failure, cardiac complications of pregnancy, and peripheral circulation in relation to pain syndromes and vascular diseases.
Brown on Edgewood Ave behind the CVRI on May 29, 1960.
When Brown officially retired from UCSF in 1979, she became a professor emeritus of medicine. Ten years later, in 1989, Brown received UCSF’s highest honor, the UCSF Medal, for outstanding personal contributions to the University’s health sciences mission.
Brown and Francis Sooy, UCSF Chancellor 1972-1982, at the time of her retirement.
Brown passed away in October of 2006 at the age of 96. At that time, she gifted over $100,000 to the UCSF School of Medicine for the improvement of teaching for medical students.
Browns’ numerous contributions over the course of fifty plus years can still be felt today– through her impact on cardiovascular research as well as her in her insight and refinement of medical education.
Contact us if you have any questions or would like to learn more. And please don’t hesitate to use the calendar on the right to make an appointment to come in and use the collections!
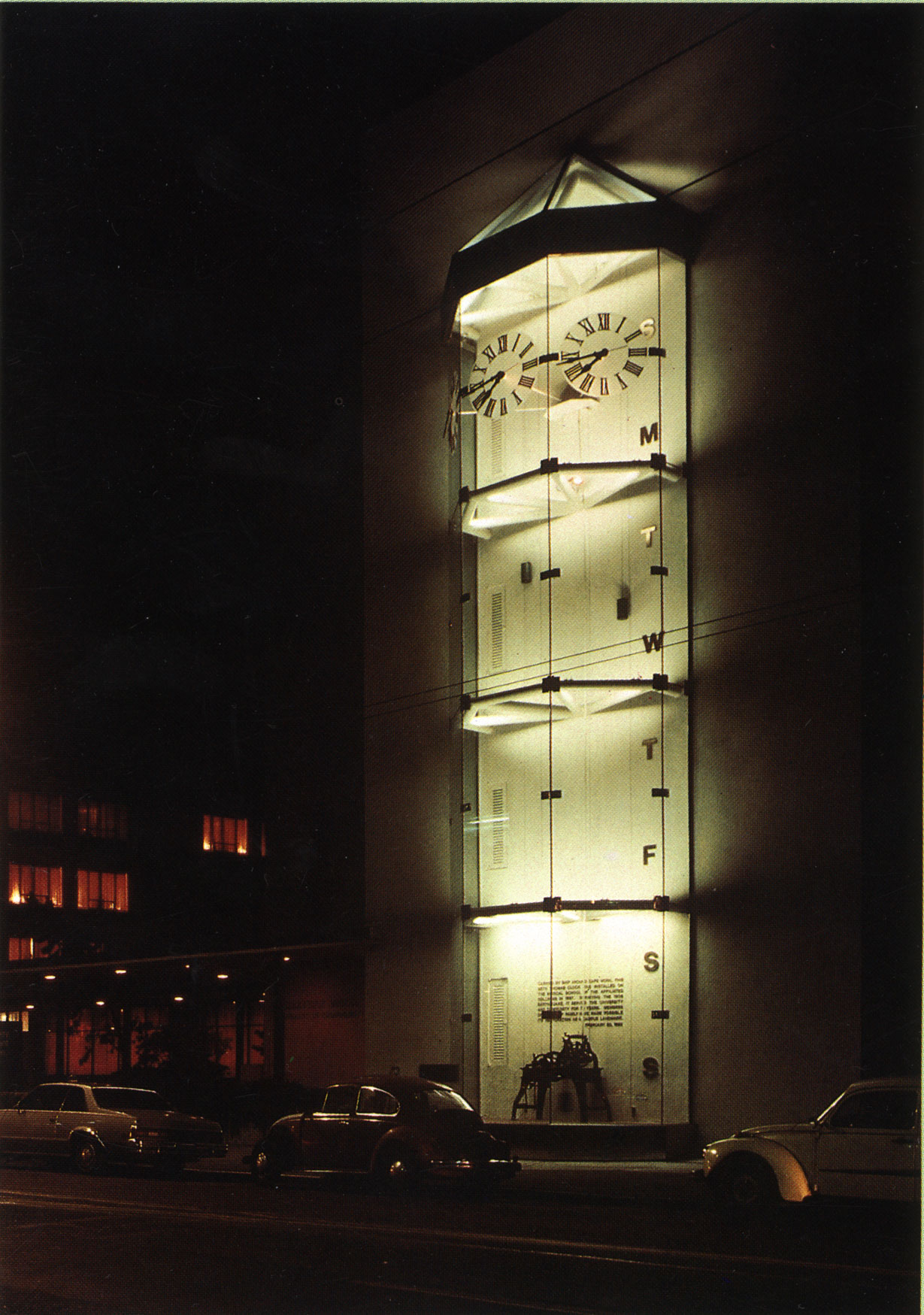
Have you ever noticed the large transparent clock on the exterior of Millberry Union? It looks like this:
I walk past it often without giving it a second thought, but the clock tower has quite an interesting history.
Often referred to now as the “Founders’ Clock,” it is also known as the “Toland Clock Tower” and “Seth Thomas Clock.” You may also have seen photographs of the Old Medical School building from time to time, with a large clock atop the center of the building– the same clock as Millberry’s clock.
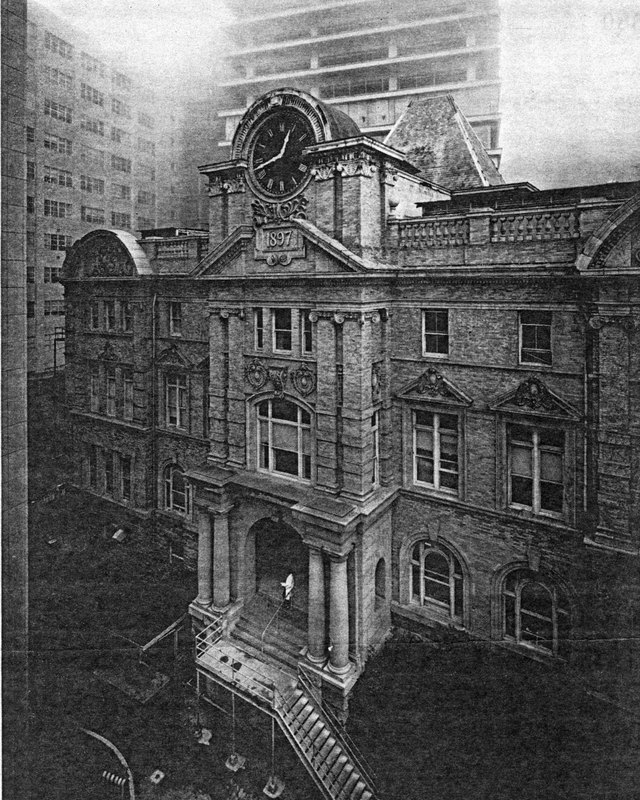
One of our rotating banner images here on Brought to Light depicts the old Medical Building, including the Seth Thomas Clock, through the lens of well-known photographer Ansel Adams. It’s a slice of this photograph:
Ansel Adams, Clock Tower of old Affiliated Colleges building, with new structures in fog, August 1964
The above building was the College of Medicine, and the first building to have been erected on the Parnassus campus in 1897. Seth Thomas was a well-known clockmaker in Connecticut in the early and mid 19th century. The clock was brought to San Francisco via ship that traveled around Cape Horn, South America to be a crown jewel in the Affiliated Colleges campus. The image, taken in 1964, shows the old College of Medicine building surrounded by the more modern campus buildings of today in the background and on the left. When the old College of Medicine building was torn down in 1967, a group of “friends of the clock”, led by Alison Saunders, MD and assisted by Meyer Schindler, MD ’38, formed to ensure it’s safekeeping until it could be moved to a new location on campus. “We have salvaged the granite pillars and blocks as well as the clock from the old building that was a landmark on Parnassus Heights . . . ,” Dr. Alison Saunders declared in 1969 as chair of the UCSF Campus Court Development Commission.
The process to find the famous clock a new home took 14 years. Finally, in 1982 the inner-workings of the clock were reinstalled on Millberry Union, 500 Parnassus Ave, where it lives today.
Founders Clock, Millberry Union, circa 1982
Next time you’re walking around the Parnassus campus, take a closer look at the historic clock. It is a work of art worthy of our attention.
The inscription reads: “Carried by ship around Cape Horn, this Seth Thomas Clock was installed on the Medical School of the Affiliated Colleges in 1897. Surviving the 1906 earthquake, it served the University and community for 70 years. Members of the UCSF family have made possible its restoration as a campus landmark.”
Check out this article that details the historical inspiration for a new clock, “Saunder’s Clock,” in the Mission Hall courtyard of the UCSF Mission Bay campus.
Join us on Monday, October 13th as M. Michael Thaler, M.D., M.A. (Hist.) gives a lecture in a series launched by UCSF Archives & Special Collections.
Date: Monday, October 13th, 2014 Time: 12 pm-1:20 pm Location: Lange Room, UCSF Library, 530 Parnassus, 5th floor This lecture is free and open to the public.
Please RSVP to reserve a seat.
Shimkin’s “Lost Colony” (1947-1953): Early Interdisciplinary Cancer Research at UCSF
Michael B. Shimkin, Director of the Laboratory of Experimental Oncology at UCSF, 1947-1953
The Laboratory of Experimental Oncology (LEO) was established in 1947 at Laguna Honda Hospital in San Francisco as a “colony” of the National Institutes of Health, to be jointly administered by the National Cancer Institute (NCI) and UCSF. The LEO was the brain child of Michael B. Shimkin, a career U.S.P.H.S. physician and cancer researcher at the NCI. Shimkin was a native San Franciscan, having successively graduated from Lowell High School, UC Berkeley and UCSF. After 8 years at the NCI and war service, Shimkin returned to his native city and alma mater as ideal environments for a “combined” interdisciplinary clinical and basic research unit embedded in a medical school and staffed by full-time research teams of M.D.’s and Ph.D.’s. These unprecedented ideas directly challenged the traditional separation between patient care and laboratory research. Shimkin introduced a ‘release’ form that fully informed patients with terminal cancer admitted to the LEO about the incurable nature of their illness, and clearly distinguished between therapeutic and experimental procedures. This prototypical “informed consent” approach met with mounting resistance from the clinical faculty. In response, Shimkin organized a symposium at UCSF in October 1951 on the subject on human experimentation. In his presentation, Shimkin became the first American physician to draw on the injunctions from the recently concluded Nuremberg trials against German physicians who had conducted medical experiments in Nazi concentration camps, as a source of universal guidelines for the ethical conduct of experiments with human subjects. The LEO treated 500 patients and generated over 130 publications before being replaced by the Moffitt-based Cancer Research Institute in 1953.
About M. Michael Thaler
M. Michael Thaler, M.D., M.A. (Hist.)
Michael Thaler received his M.D. from the University of Toronto, trained in pediatrics, pediatric pathology and internal medicine, and completed research fellowships in cell biology at Washington University and in developmental biology at Harvard University. As professor of pediatrics at UCSF, he established the first academic division of Pediatric Gastroenterology, Hepatology and Nutrition in North America, was awarded the first NIH Research Career Development Award in Pediatric Gastroenterology, and was P.I. of the foundational NIH Research Training Program grant in Pediatric Gastroenterology. He also directed the Laboratory of Pediatric Hepatology and served as associate director of the UCSF Liver Center. His publications include approximately 200 clinical and basic research articles on perinatal bilirubin metabolism, infantile cholestasis syndromes, Reye’s syndrome, and bile salt metabolism. As professor emeritus, he earned a M.A. degree in History of Health Sciences at UCSF in 1998, and received appointments as Visiting Scholar at the Stanford Center for Bioethics, and Research Associate at the Stanford Center for History and Philosophy of Science. For the next 12 years, he taught undergraduate courses on the history of medical sciences as Visiting Professor of History at UC Santa Cruz and UC Berkeley. He continues to lecture at the Osher Life Long Learning Institute in Berkeley, and for the fellowship program in Pediatric Gastroenterology at UCSF. His awards include the UCSF Chancellor’s Faculty Award for Public Service and the Shwachman Lifetime Achievement Award in Pediatric Gastroenterology. He presently serves as president of the UCSF Emeriti Faculty Association.
About the UCSF Archives & Special Collections Lecture Series
UCSF Archives & Special Collections launched this lecture series to introduce a wider community to treasures and collections from its holdings, to provide an opportunity for researchers to discuss how they use this material, and to celebrate clinicians, scientists, and health care professionals who donated their papers to the archives.
Within 18 years of California Statehood in 1850, the University of California was established in Oakland (1868). Already well-known in San Francisco were 2 private medical colleges, Cooper Medical College, which later was aligned with the University of the Pacific and then became the Stanford School of Medicine, and Toland Medical College, which first offered classes in 1864. Within 9 years (1873), Hugh Toland gifted the University of California with the school buildings and property in North Beach across from the San Francisco City and County Hospital. Continue reading →