By Erin Hurley, User Services and Accessioning Archivist
We are currently more than halfway through Black History Month, a month that takes on special significance this year, following a summer of protests asserting, yet again, that Black Lives Matter. Archives & Special Collections would be remiss if we failed to mention the groundbreaking Black faculty at UCSF, both past and present, who have made significant contributions to the fields of medicine and psychology (as well as many others), and, who, in their work, have found ways to illuminate new facets of racism previously unconsidered and who, on their paths to success, have also sought to support and lift up others.
Mindy Thompson Fullilove is a social psychiatrist who served as Assistant Clinical Professor of Psychiatry at the UCSF Center for AIDS Prevention Studies (CAPS) from 1983 until 1990. Her work sits at the intersection of mental health and public health, and she focuses, in her own description, on the “sources and consequences of inequality, with a focus on the American city,” including segregation, gentrification, and the impact of these forces on the mental and physical health of Black families. [1] She is the author of numerous books, including The Black Family: Mental Health Perspectives and Root Shock: How Tearing Up City Neighborhoods Hurts America and What We Can Do About It.[2]Most recently, she has co-edited a volume titled From Enforcers to Guardians: A Public Health Primer on Ending Police Violence. In 2018, she gave a TED talk which gives an overview of her work and her personal history and outlines her hopes for achieving equality.
Mindy Thompson Fullilove
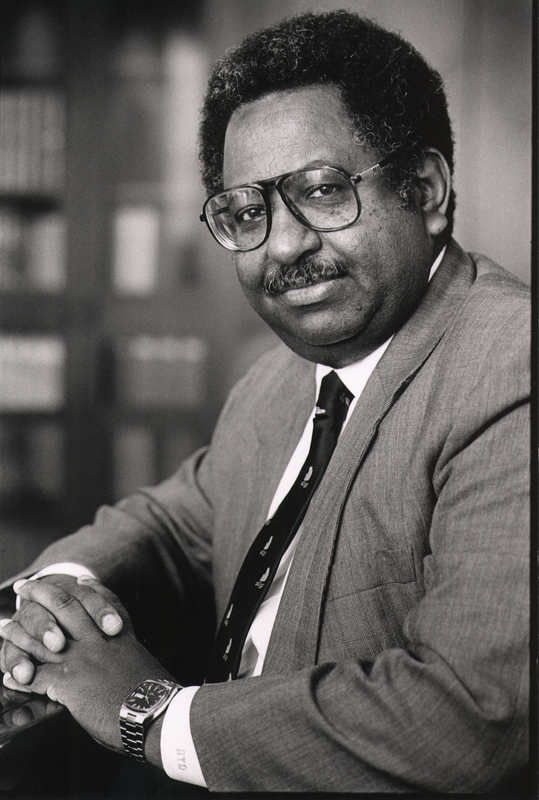
Eritrean surgeon Haile T. Debas has, many times over, served as an example of what Black leadership can look like, and has shown how it can benefit others in a variety of ways. Debas, who came to UCSF in 1987 to serve as the Chair of the Department of Surgery, specializes in gastrointestinal physiology. During his time as Chair, UCSF “became one of the country’s leading centers for transplant surgery, the training of young surgeons, and basic and clinical research in surgery.”[3] He then went on to serve as the Dean of the School of Medicine for 10 years, from 1993-2003. In 1997, he was appointed as the 7th Chancellor of UCSF, a position that he agreed to hold for one year while also serving as Dean of the School of Medicine.
Haile T. Debas, photo courtesy of UCSF University Relations
Debas, in his long and distinguished career, has demonstrated a commitment to serving underserved areas, from his work in the Yukon Territories, where he practiced surgery early in his career, to a long-held dream of establishing a medical school in Eritrea. It was this commitment that led him to establish, in 2009, the UC Global Health Institute, which sought to leverage the expertise and resources of all ten UC campuses to address global health issues, which he says are “so big that single disciplines can’t tackle them.”[4] He also served as Executive Director of UCSF Global Health Sciences (GHS), established in 2003, which focuses on issues like diseases of poverty, chronic illnesses, and the global threat posed by certain infectious diseases, like COVID-19.
His work in global health has informed his support for women’s empowerment movements, and he notes, “In global health, women’s empowerment is the critical element—nothing will be accomplished to a successful end without women’s support.”[5] Debas also established the UCSF Department of Surgery’s Haile T. Debas Diversity Fellowship for Fourth Year Medical Students, which offers fourth year medical students a sub-internship in the Department of Surgery, as well as a $2,500 stipend.[6] Debas appears often in Archives & Special Collections materials, as a part of the Office of the Dean’s records, as well as in the Global Health Sciences records and the Oral History collection.
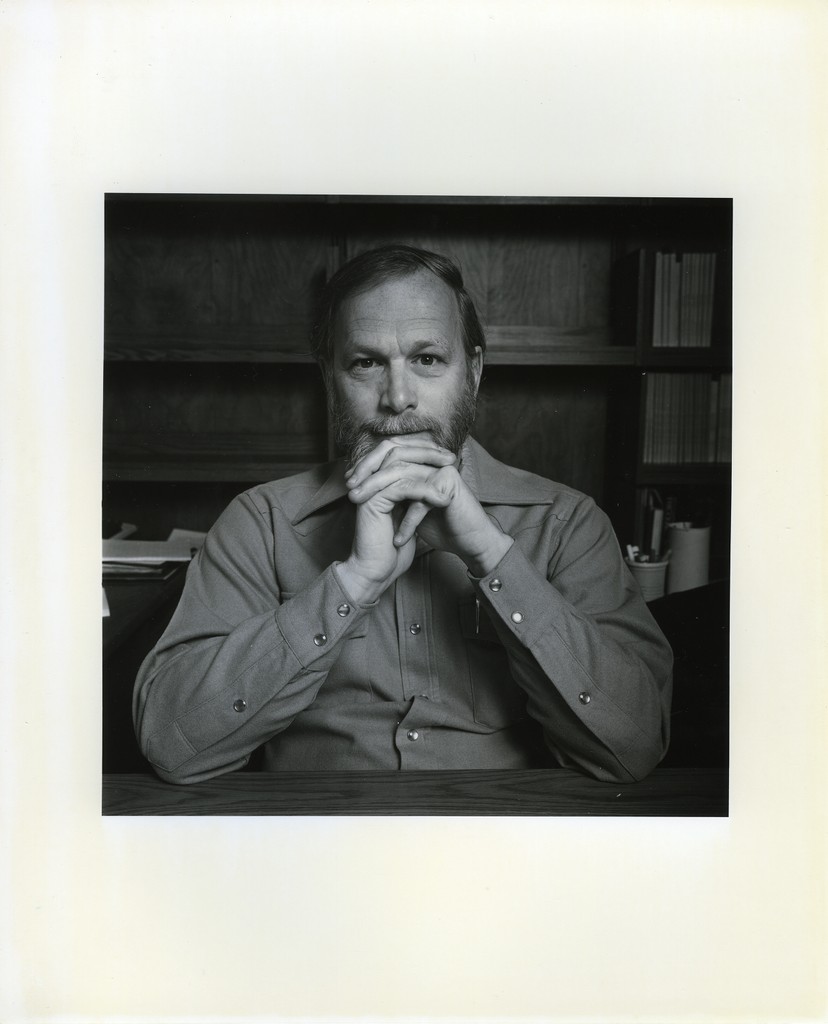
UCSF Archives and Special Collections is pleased to announce that 93 cartons have been processed and added to the J. Michael Bishop papers. The collection was first processed in 2016 with a total of 19 cartons, it grew to 142 linear feet. The new material includes lectures, correspondence, memorabilia, and committee files. The collection’s finding aid is available publicly on the Online Archive of California.
J. Michael Bishop portrait at desk. J. Michael Bishop papers, MSS 2007-21, carton 19, folder 52
Bishop is the recipient of numerous awards in addition to the Nobel Prize, including the Albert Lasker Award for Basic Biomedical Research and the American Cancer Society National Medal of Honor. In 1989, Bishop and his colleague, Harold E. Varmus, were awarded the Nobel Prize in Physiology or Medicine for the discovery that growth regulating genes in normal cells can malfunction and initiate the abnormal growth processes of cancer.In 2003, he was awarded the National Medal of Science. On July 1, 1998, J. Michael Bishop became eighth chancellor of UCSF, and presided over what would become the largest academic biomedical expansion in the nation-the creation of the UCSF Mission Bay campus.
Nobel Attire cartoon. J. Michael Bishop papers, MSS 2007-21, carton 6, folder 31
The collection is arranged into twelve series which include: Series I. Writings and publication files; Series II. Teaching files; Series III. Laboratory research notebooks and binders; Series IV. Working files; Series V. Scrapbook and artifact; Series VI. Exhibit files; Series VII. Committee files; Series VIII. Correspondence; IX. Postdoctoral files; X. Meetings and Travel files; XI. Lectures and Remarks; XII. Photographs, Slides, and Audio/Visual Material.
You can view the collection’s finding aid and many other UCSF collections’ finding aids on the Online Archive of California.
This is a guest post by Aaron J. Jackson, M.A, Ph.D. Candidate, UCSF History of Health Sciences.
From time to time, events in the
present so closely resemble events from the past that the aphorism “history
repeats itself” seems feasible. This can be demonstrated by comparing the
current crisis of the novel coronavirus with the influenza pandemic of 1918-1919.
The similarities are compelling. Like the SARS-CoV-2 coronavirus, the variety
of H1N1 influenza that swept across the world in 1918 and 1919 produced a
significant shock. It spread like wildfire, was frustratingly resistant to
contemporary therapeutics, exhibited novel characteristics, and forced
governments to resort to what some considered to be heavy-handed public health
interventions. Bay Area residents in 1918 were required to wear masks and
practice social distancing, just as they are required to do so today. Such
historical similarities are not, however, proof that history repeats itself.
But they do provide interesting opportunities for comparison between the past
and the present—opportunities that hold the potential to make the past more relatable
by building connections through common circumstances. And perhaps, through that
understanding, an opportunity for hope to shine in dark times.
This post is not an exhaustive
study comparing 1918 and 2020. Rather, it focuses on responses to crises and
specifically the ways that communities innovatively addressed shortages of
personal protective equipment (PPE). So, of course, it will be about war,
pandemics, socks, and sheet protectors. Naturally.
When the United States declared
war on the Imperial Government of Germany in April 1917, the nation was
woefully unprepared for the conflict. The war represented an unprecedented
crisis—one that required the federal government to assume new powers in order
to coordinate the resources of the entire nation. President Woodrow Wilson’s
administration worked with Congress to institute a draft to raise an army,
enacted strict economic control measures to conserve and direct resources
towards the production of war materiel, and passed laws that infringed on civil
liberties, all in the name of the war effort. To ensure public support for
these moves, the government mounted a massive propaganda campaign that appealed
to a specific version of American patriotism, appealing to citizens’ sense of
duty.
Mustering an army of sufficient size presented significant challenges. The men not only had to be inducted into military service—either by volunteering or being drafted—they required hundreds of training camps, transportation to those camps, equipment to train with, uniforms to wear. Once at the camps, they required food, shelter, and medical support. Military training was and remains a dangerous business, but the most significant medical problem at the cantonments was disease.
Base Hospital No. 30 “Officers and Enlisted Personnel” from the Woolsey (John Homer) Papers, MSS 70-5, UCSF Archives and Special Collections
As tens of thousands of American
recruits assembled at Army camps across the United States, they unwittingly
brought diseases with them, which found ample opportunity to spread in cramped
camp conditions. Most of these infections fell into the category of “common
respiratory unknown disease”—an unofficial designation among military recruits
who learned to add C.R.U.D. to the lexicon of military acronyms they learned.
The crud largely consisted of the common cold and other respiratory infections,
but cases of measles, mumps, and chicken pox were also common. Most cases of
the crud cleared up without need for treatment, but the prevalence of these
infections and the fact that new waves of infections would spring up with every
new trainload of recruits had the effect of masking a more dangerous threat.
Army physicians first identified more than 100 soldiers who had developed a
rather severe flu-like illness in March 1918. Within a week, the number of flu
cases at Fort Riley was over 500 and climbing. The H1N1 virus that caused the
influenza pandemic of 1918-1919 had arrived, but the nation was focused on the
war. And as American troops began arriving in France and moving into the front
lines—many of them no doubt bringing the virus with them—medical personnel
tasked with supporting the war effort shifted their focus from induction
screening and camp illnesses to other health concerns.
The First World War introduced a bevy of new ways to mangle and maim human bodies. From high-velocity rifle rounds and machine guns to high-explosive artillery shells, flamethrowers, hand grenades, aerial bombardment, and chemical weapons, the U.S. Army Medical Corps understood that the hospital system it established in France had to be prepared first and foremost for trauma care, which posed significant challenges. Not only did modern weapons cause extensive damage, the risks of sepsis and gangrene in an era before the discovery of antibiotics were high. Complicating this, European battlefields tended to stretch across agricultural land, teeming with bacteria after years of fertilization. Soldiers wounded on the front lines thus ran an extremely high risk of bacterial infection. To address this, the Medical Corps and its affiliates prioritized training Army health care workers in antiseptic wound care.
“U.S. Army Base Hospital No. 30, World War I (University of California School of Medicine Unit),” from The Thirtieth, AR 207-16, UCSF Archives and Special Collections
The experiences of the personnel of Base Hospital No. 30 are instructive in this regard. Base Hospital Thirty was the military hospital unit assembled from physicians, surgeons, and nurses associated with the University of California’s School of Medicine—the precursor to UCSF. Organized with the help of the American Red Cross Society shortly after Congress declared war, the unit spent more than a year training for the anticipated challenges of running a hospital for wounded soldiers in France. The unit’s nurses received orders to depart San Francisco on December 26, 1917 and reported to Army cantonment camps along the East Coast to help care for soldiers who had fallen ill with the crud, gaining invaluable experience in nursing soldiers and recognizing disease presentation. The unit’s surgeons practiced the ancient technique of wound debridement—removing foreign objects and cutting away dead and dying flesh to produce a clean wound—and attended clinical instruction that prepared them for the types of injuries they would face. And the unit’s corpsmen trained in the production and use of the Carrell-Dakin solution, a novel antiseptic more effective than carbolic acid and iodine but also a solution that required careful training and preparation. Thanks to training like this, the base hospital system was able to treat more than 300,000 sick and wounded soldiers with remarkably low mortality rates compared to previous wars.
Indeed, the medical apparatus and personnel organized to support the American Expeditionary Forces were well prepared for the anticipated hazards of the war. But in one of the remarkable parallels to the current coronavirus crisis, their job was perhaps made more difficult by the failure of American logistics in providing adequate personal protective equipment. But the shortage in 1918 was not one of N95 masks; rather, it was a matter of needing socks.
Today, the Occupational Safety
and Health Administration defines PPE as “equipment worn to minimize exposure
to hazards that cause serious workplace injuries and illnesses.”[i]
Under this definition, and in the context of soldiering, a good pair of socks
certainly applies. Trench warfare was a dirty business. It also tended to be
cold and wet—the perfect climate for a condition known today as “trench foot.”
Afflicted soldiers’ feet would go numb, swell, develop sore and infections, and
in extreme cases become gangrenous, possibly requiring amputation. Obviously,
this ran the risk of keeping soldiers from the front lines and thus undermining
the war effort. But ensuring a plentiful supply of clean dry socks somehow
slipped through the cracks of the Army’s logistical efforts to prepare for the
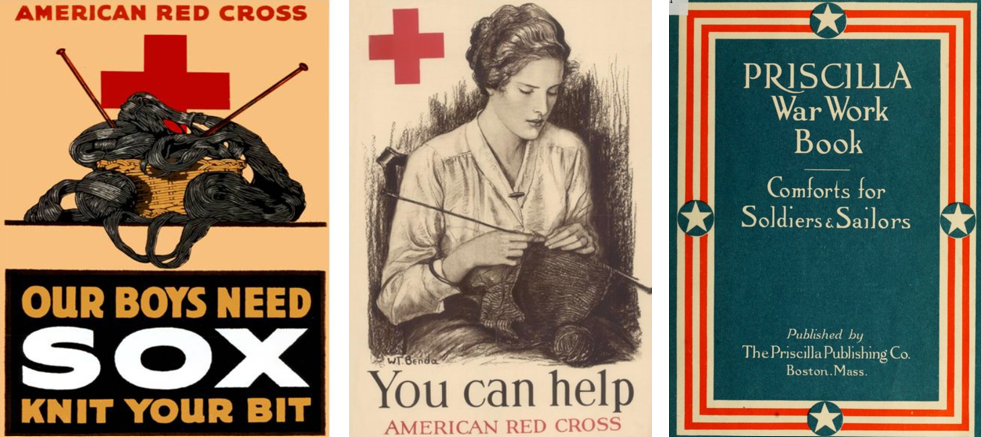
war. Fortunately, the American Red Cross and thousands of civilian volunteers
found ways to meet the challenge.
Beginning in 1917, the Red Cross put out calls for knitted garments, especially socks. The organization distributed officially-endorsed knitting patterns and free wool to anyone willing to “knit your bit.” The Priscilla War Work Book contains roughly a dozen such patterns ranging from socks to coats and winter hats.[ii] But the demand was greatest for socks. Across the country, knitters worked individually at home and collectively in social groups to try to keep up with the demand. Those who could not knit were urged to purchase or donate wool for the cause. Some organizations turned to mechanical solutions. The Seattle Red Cross utilized a knitting machine to produce long wool tubes that could be cut into 27-inch lengths, requiring only the toes to be stitched by hand.[iii] In this way, those behind the front lines were able to support the war effort by providing the PPE the soldiers needed to keep themselves in fighting shape.
Celebrating the end of the First World War in San Francisco, November 11, 1918. Image from The San Francisco Chronicle files.
Celebrating the end
of the First World War in San Francisco, November 11, 1918. Image from The San Francisco Chronicle files.
The knitting campaign continued
until the war ended with the declaration of the armistice on November 11, 1918.
By then, the nation was in the midst of the first wave of the influenza
pandemic. On October 9, 1918, San Francisco’s hospitals reported 169 influenza
cases. A week later, there were more than 2,000 and the city’s Board of Health
issued recommendations for social distancing.[iv]
With so many health care professionals supporting the war effort, the Bay
Area’s medical infrastructure was stretched to the limit and cities put out
calls for volunteers. Hospital space soon became a valuable commodity and many
facilities, including the Oakland Municipal Auditorium, were converted into
temporary hospitals, and public health officials began recommending the use of
face masks, which they later made mandatory.[v]
But it is important to remember that these were local efforts to respond to the
pandemic. The federal government, which had mustered the resources of the
entire nation to fight the war in Europe, was unwilling to do the same to
combat the pandemic at home, leaving it up to local authorities, medical
institutions, and volunteer organizations to make do as best they could.
“Oakland Municipal Auditorium is used as a temporary hospital,” 1918, Oakland Public Library
Unfortunately, we find ourselves
in a similar situation today. As the novel coronavirus took on pandemic
proportions, stores of PPE for frontline healthcare workers reached critical
levels. Before the pandemic, China produced approximately half the world’s
supply of medical masks. As the infection spread in China, their exports
stopped, and the resulting shortage spurred competition between institutions
and governments to secure PPE, which only exacerbated the situation.
Thankfully, a multidisciplinary team at UCSF found a way to be a part of the
solution, echoing the efforts of American knitters from over a century ago.
From left to right: UCSF shield frames,; A completely assembled UCSF face shield; Dr. Alexis Dang wears an assembled face shield over a N-95 respirator. For additional information please read the UCSF Library Makers Lab story. UCSF Library Makers Lab Left to right: UCSF shield frames,; A completely assembled UCSF face shield; Dr. Alexis Dang wears an assembled face shield over a N-95 respirator. For additional information please read the UCSF Library Makers Lab story
Noting the need for face shields, experts at UCSF specializing in biochemistry, engineering, logistics, medical workplace safety, and 3D model design came together in March 2020 to develop something that could help address the PPE shortage. By April, the team completed designs for three different models of 3D-printable face shield frames that, when combined with rubber bands and transparent document protectors, serve as functional and reusable face shields. They then collected seventeen 3D printers from across the university and turned the UCSF Makers Lab in the Kalmanovitz Library into an ad hoc face shield factory that can produce more than 300 shields each day—enough to supply UCSF’s front-line health care workers and then some.[vi] Extra shields are distributed to Bay Area hospitals. Moreover, like the Red Cross with the distribution of the Priscilla War Work Book, the UCSF team is sharing their plans in an open source repository so that others can emulate their efforts.[vii] This allows those with access to 3D printers and a few dollars’ worth of office supplies to contribute to the ongoing PPE shortage by producing face shields that have been designed, tested, and vetted by experts at one of the nation’s leading medical institutions.
Certainly, there are remarkable
similarities to be drawn between the modern crisis and those in the past. Once
again, the government was unprepared for a crisis despite advanced warning.
Once again, people are working in the front lines to save others despite
inadequate supplies. And once again, like the First World War and the influenza
pandemic of 1918-1919, the coronavirus pandemic is a devastating event likely
to be measured in the tally of lives lost. In the face of such grim statistics,
it is easy to fall into cynicism and say that history is repeating.
In 1905, philosopher George
Santayana explored the notion of progress—the idea that things move toward
improvement—and stated that “those who cannot remember the past are condemned
to repeat it.”[viii]
This is likely the origin of the aphorism “history repeats itself.” But Santaya
was not making a hopeless argument; rather, he noted that if progress is to be achieved,
it will be because humans not only record the past, they engage with it, learn
from it, and seek to understand it. And how that is achieved depends on the
ability to draw relatable connections with the past that emphasize human
agency. In 1918, knitters took up their needles. Today, a team of scientists,
engineers, and others figured out how to make face shields using 3D printers
and office supplies. These may seem like small contributions in the grand
scheme of things, but they are important examples of positive human agency in
the face of crisis.
[ii]
Elsa
Schappel Barsaloux and the American National Red Cross, The Priscilla War
Work Book: Including Directions for Knitted Garments and Comfort Kits from the
American Red Cross, and Knitted Garments for the Boy Scout. Boston, Mass.:
The Priscilla Publishing Company, 1917. Available at the HathiTrust Digital
Library. https://hdl.handle.net/2027/loc.ark:/13960/t2988wd21
[iv]
“Thirty-Seven New Cases Found in S.F.,” San Francisco Chronicle 10 Oct.
1918, 3; “Hassler Urges Churches and Theaters to Close,” San Francisco
Chronicle 17 Oct. 1918, 5.
[v]
“Wear a Mask and Save Your Life!” San Francisco Chronicle, 22 Oct. 1918.
Robert E. Allen, Jr., MD, (1935-2018), was born in Blountstown, Florida and always aspired to become a doctor. In pursuit of his dreams, Allen received a bachelor’s degree in Biology from Florida A&M University, master’s degree in Genetics from Michigan State University, and a doctorate in Medicine from Meharry Medical College. He completed his residency in surgery at UC San Francisco, and a fellowship in surgery oncology at Memorial Sloan-Kettering Cancer Center in New York City. Allen also completed two additional postdoctoral fellowships in surgery at the National Institute of Health and peripheral vascular research at San Francisco General Hospital. As a SFGH fellow in trauma, he organized the ambulance paramedic program while training under F. William Blaisdell, MD.
Robert Allen Jr., David Powers collection, 1990-1991
Dr. Allen began his career at UCSF as a Surgical Oncologist,
specializing in Melanoma Surgery. He soon became the first Black Clinical
Professor of Surgery at UC San Francisco, serving as a faculty member for over
four decades.
Allen was a cofounder of the Northern California Melanoma
Center with Dr. Lynn E. Spitler and other surgeons. Here, he participated in
consultation panels and surgeries on the Center’s patients until his
retirement.
He has authored many articles for medical periodicals, wrote
chapters in medical publications, and spoke a medical conventions throughout
the United States and Europe. In addition, he was a member of various honor
societies, including the UCSF Naffziger Surgical Society.
To learn more about Dr. Allen’s work, check out these articles:
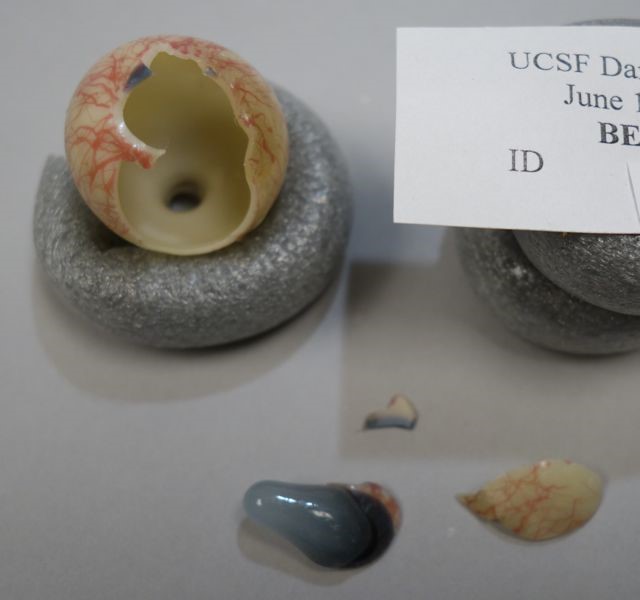
Since 1963, the UCSF Archives & Special Collections holdings
have included the historic Danz collection of ocular pathology specimens. The
set, one of 13 believed to have been made, was originally intended as a
teaching tool for use in medical schools. These blown orbs, some still retaining
a long delicate stem, were made in Germany, in the 1880’s, by master
glassblower, Amandus Muller. Each glass eyeball depicts, in minute detail, the
various diseases and defects that can afflict the eye and is a unique
masterpiece of the art of glass making.
In June 2018 the collection was examined by Tracy Power and Lesley Bone to determine the nature and scope of condition problems that these objects. Past treatments and current breakages were evaluated, the deterioration of the glass was examined, and current storage conditions were assessed.
While the majority of the glass eyeballs were in stable
condition, there were ironically a couple that were themselves suffering from
glass disease. This presents with a sticky surface; as a component of the glass
leaches out of the surface due to an instability in the glass mix. These
surfaces readily attract dust.
Of the previously repaired items, some were in stable
condition, but most were in poor condition due to deterioration of the repair
materials used and inferior skills of the person or people doing the repairs. One
particularly peculiar repair was filled with bright red dental wax.
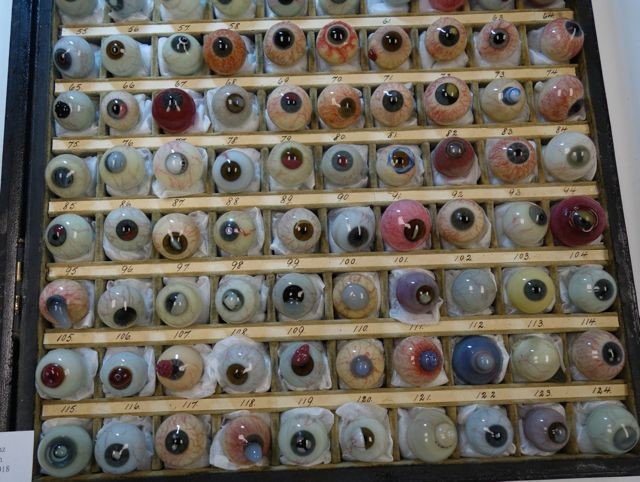
The eyeballs were stored in their original compartmented box, with light damaged (faded), velvet-covered cavities for each specimen, and a hinged lid with a glass cover. The box was still serviceable, but the cavities for the eyeballs had wads of old cotton wool, which was not suitable for the collection since the blown balls retained the thin tubular glass extensions that had been snapped from the rod when the ball was blown. These tended to snag on the cotton.
A treatment plan was agreed upon which would include
upgrading the storage container, cleaning all of the glass eyeballs, and
repairing the broken glass orbs.
Improved Housing
The eyeballs were removed
sequentially for cleaning, and at that time the cavities in the display box
were cleaned and new, improved supports were made. The old cotton wool was replaced with new
storage materials that will not be as likely to snag the glass tips. Small pillows were made of polyester batting
in Holytex fabric. The glass pane in the
box was cleaned with detergent and water.
Several discolored areas of paper on the box were toned with conservation
stable watercolors and some lifting edges of paper were glued down.
Old cotton wool was removed and replaced by individually made pillows of archival materials.
Cleaning of the glass eyeballs
Each glass eyeball was
carefully cleaned. A detergent designed
specifically for cleaning glass was used for this process. Handling the eyeballs safely was a major
concern and we ended up using foam tubes to make little doughnuts for the glass
balls to sit in. The foam was held in
place with toothpicks, so their creation and adjustment was relatively quick.
During the cleaning we identified some additional cracks in the glass eyeballs
that hadn’t been obvious until they were wet up. This step was very satisfying as the eyeballs
went from dull and cloudy to glistening after cleaning.
Cleaning the glass and the compartments in the box.
Repairing of Glass Eyeballs
Before the eyeballs could be repaired,
those with unsightly or failing old repairs had to be undone. The method varied depending on the types of
repair materials previously used.
Several of the repairs had been done with red wax. The wax remained soft and sticky making it
messy and it did not closely resemble glass.
The wax material was removed by gently warming it. Some of the other old adhesives had failed after
becoming brittle. The brittle material
could be brushed from the surfaces, with special care taken to not scratch the
glass. Other old repair materials were
removed with solvents.
Old repair with red wax
Old repair with red wax
Old repair undone and redone with improved materials and techniques
Old repair with pieces misaligned
Disassembled and repaired in proper alignment
Repairing
the individual eyeballs was the most challenging part of the process, as they
are thin and delicate. Added to that,
the high-grade epoxy that was designed for glass conservation can take several
days to fully set. While this can be advantageous,
as it allows adjustment of pieces, it also means the fine shards have to be
held in place for long periods of time while the resin sets. An advantage of
this epoxy is that it is very thin and can be fed by capillary action into
cracks. That property was useful for
many of the eyeballs. Also this adhesive has the added advantage of being far
superior to commercially available epoxy resins in terms of long-term stability
and greater light-stability, therefore it does not yellow like commercially
available epoxies.
Before treatment
After cleaning and gluing
Before treatment
After cleaning and gluing
Once the eyeballs were repaired, a few had areas where the fragments of the glass were still missing. Glass eyeballs that were incomplete were filled with tinted thermoplastic resin mixtures and details such as veins, were inpainted (inpainting is the process of restoring lost or deteriorated surface decoration or details on an artwork) with commercially ground pigments in acrylic resin.
Before treatment, misaligned and losses
Old repairs undone
Treatment completed with pieces glued together and area of loss filled and veins inpainted on the fill
Eyeball before treatment, in pieces but with some old repairs still intact
After removing old repairs
Pieces glued together and held with tape. Area of loss remained
Area of loss after gluing all pieces together
After repair, glued together and area of loss filled with tinted resin mixture
After repair showing area that was filled
The glass eyeballs were incredible to work on. They were beautifully made, if often difficult to look at. Only one of the eyeballs examined was failing due to unstable glass, or a poor match between the cream under layer and the colored surface glass. The glass blower had incredible mastery in working with glass in addition to skill in depicting the defects and conditions. We hope that after this conservation project the glass eyeballs continue to illustrate medical conditions and inspire awe for years to come.
UCSF Archives and Special Collections is pleased to announce that the Arthur E. Guedel Anesthesia Collection is now processed. The collection’s finding aid is available publicly on the Online Archive of California. Collection processing made possible through support from the Arthur E. Guedel Memorial Anesthesia Center Board of Trustees.
Arthur E. Guedel, MSS 2016-03, carton 12, folder 5
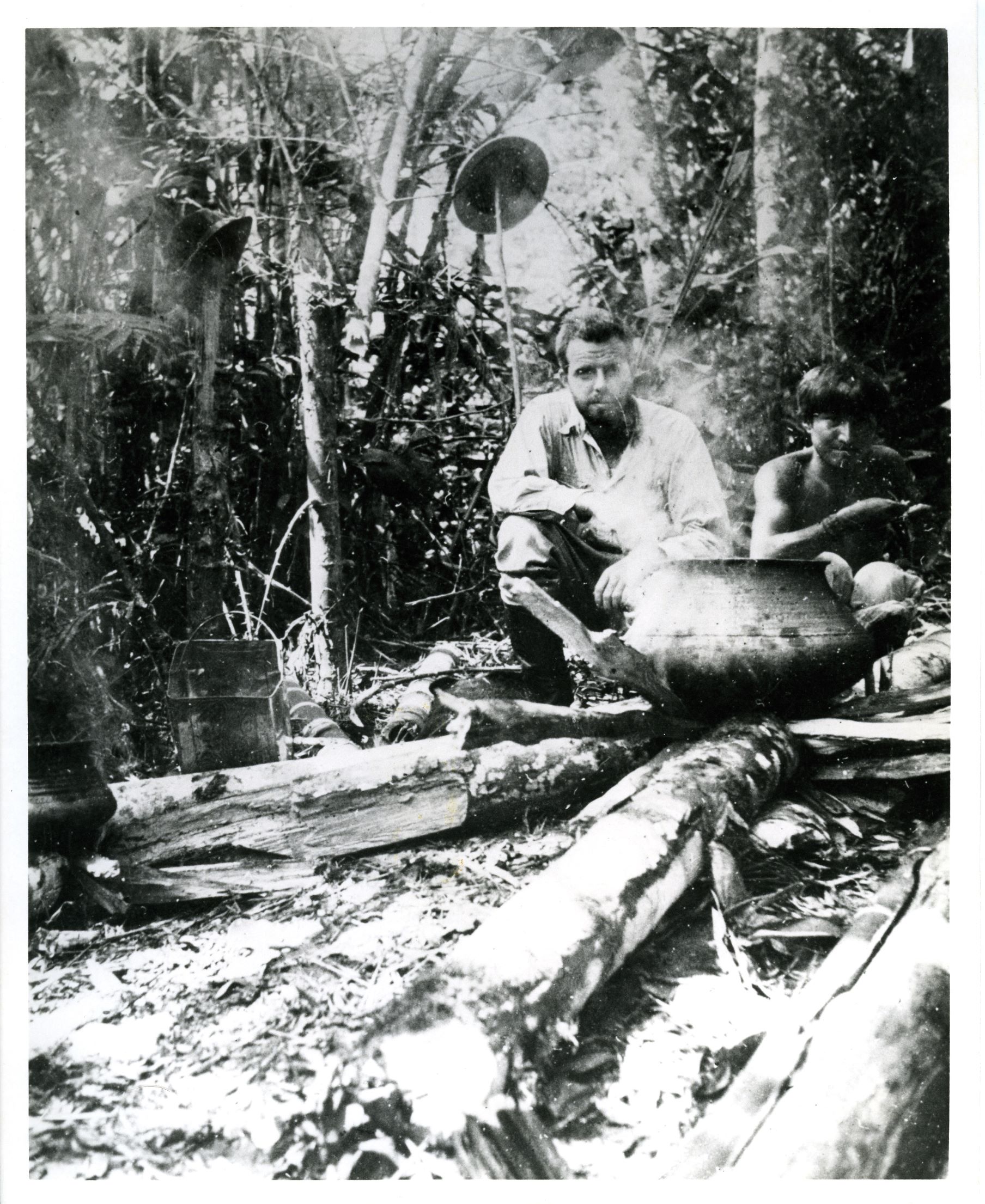
Arthur E Guedel, M.D., was an anesthesiologist and clinical professor of anesthesia at the University of Southern California. The collection documents Dr. Guedel’s long career as an anesthesiologist. The collection includes a variety of material related to his research and his professional service. The collection also includes material from Dr. A.E. Bennett, Dr. William Neff, Dr. Leonard Ramsay Thompson, and Dr. Richard C. Gill’s Ecuadorian curare expedition. The collection also includes material from the Guedel Memorial Anesthesia Center and includes administration files, photographs, and correspondence.
Material in this collection relates to Guedel’s work and others in the anesthesia field, including files regarding anesthesia, anesthesia machines and equipment, ether, chloroform, curare, and other related topics. Material includes correspondence, reports and publications, files related to conferences and meetings, photographs, audiovisual recordings, artifacts, computer media, and other material.
Richard Gill Making Curare with Ecuadorian Native, MSS 2016-03, carton 12, folder 19
You can view the collection finding aid on the Online Archive of California. If you would like to visit the UCSF
Archives and Special Collections and work with the complete physical
collection, please make an appointment with us.
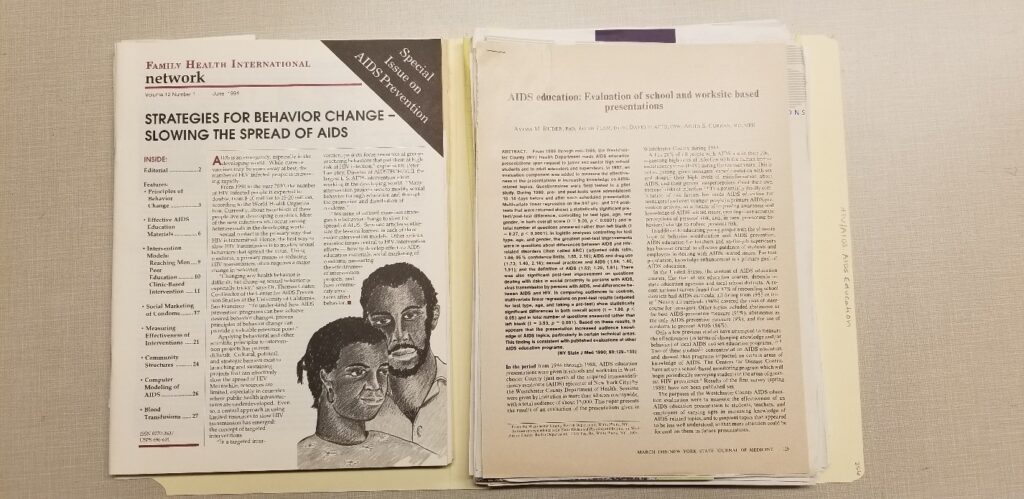
Garrett is a Peabody, Polk, and Pulitzer Prize-winning journalist. The collection features her research on HIV/AIDS and public health, correspondence, memorabilia, photographs, book and article drafts Garrett won the Pulitzer Prize for Explanatory Journalism for her work chronicling the Ebola virus in Zaire published in Newsday. She is also a bestselling author of the book The Coming Plague: Newly Emerging Diseases in a World Out of Balance. Garrett has worked for National Public Radio, Newsday, and was a senior fellow for The Council of Foreign Relations. She has won many awards including the Award of Excellence from the National Association of Black Journalists and the Bob Considine Award of the Overseas Press Club of America. Researchers are already using the collection and have found great interest in her work.
AIDS Education, MSS 2013-03, carton 25, folder 6
The collection is organized into seven series which include research and subject files, correspondence, newsletters, Betrayal of Trust: The Collapse of Global Public Health and The Coming Plague: Newly Emerging Diseases in a World Out of Balance drafts and notes, conferences, non-print material, correspondence, and memorabilia
Scrapbook, MSS 2013-03, oversize box 104
You can view the collection finding aid on the Online Archive of California. If you would like to visit the UCSF Archives and Special Collections and work with the complete physical collection, please make an appointment with us.
This is a post from intern Harold Hardin, working on the NEH grant-funded project The San Francisco Bay Area’s Response to the AIDS Epidemic.
Sue Rochman papers, GLBTHS 2005-13 miscellaneous research papers
The Sue Rochman Papers (Collection 2005-13 at the GLBT Historical Society) contain critical information regarding the systematic oppression of incarcerated people living with HIV/AIDS in the first decade of the epidemic. The collection at just over 350 pages consists of interviews, newspaper clippings, and often most compellingly, correspondence from incarcerated people living with HIV/AIDS. Given the ongoing wave of HIV criminalization (a recent famous example being the case of Michael Johnson, who, incidentally, was released this month after spending five-years of a thirty-year sentence in Missouri, for allegedly seroconverting several partners with HIV without revealing his HIV-positive status) Micheal Johnson and Greg’s Smith’s cases among others were rallying cries for HIV/AIDS activists bringing to our collective attention the ongoing histories of HIV criminalization. It is particularly important to look back at the particular ways in which this stigmatization of people living with HIV/AIDS began within the prison system and consider an early case of which the Sue Rochman Papers document. In this way, we can further contextualize our current historical moment in regards to the continuing criminalization of people living with HIV/AIDS–particularly the ways in which black gay men are overwhelmingly impacted by this deleterious trend. The correspondence between Ms. Rochman and various incarcerated people in several different prison locations (Attica prison in New York, Chino prison in California among others) echo similar findings. The correspondence notes the systematic way in which prison officials valued “security” to the detriment of the lives of incarcerated people living with HIV/AIDS. Confidentiality rights regarding seroconversion status were routinely trampled and ignored at the behest of prison officials. There was little to no basic health information regarding the spread of the disease. Incarcerated people with HIV/AIDS were often isolated in poor conditions, with little medical attention by qualified specialists in HIV/AIDS. The widespread abuse of incarcerated people with HIV/AIDS by prison guards themselves was also well documented. Having the disease in prison not only meant living in such conditions but additionally meant being socially ostracized through officially sanctioned segregation–barred from participation in vocational programs, college classes, and not allowed to have family visits. A jail in Fort Worth, Texas went as far as mandating LGB incarcerated populations wear colored wrist bands to identify their sexual orientation from afar. From such systematic forms of discrimination it is unsurprising then that HIV criminalization was birthed in such an environment. The Rochman papers document the case of Greg Smith who in 1990 was convicted of attempted murder, assault and terroristic threats. Charges were filed after he allegedly bit and spat on a guard in a New Jersey jail in 1989. He maintained his innocence throughout the trial famously saying after his sentence was read, ‘I never bit an officer, and I’ll say that until the day I die. I may die in the next year or two, but I’ll die proud. I told the truth.” His case was taken up by ACLU via ACT UP prison-activist Judy Greenspan and a significant amount of Rochman papers covers Greenspan’s media campaign and legal filings. Smith, who ultimately died in prison in 2003, was an ACT UP activist, black and gay. His case is viewed as an early example of the compounding effects of race, class, sexual orientation and HIV status-indeed of HIV criminalization.
This is a guest post by intern Harold Hardin, who is working on the NEH Grant-Funded Project The Bay Area’s Response to the AIDS Epidemic.
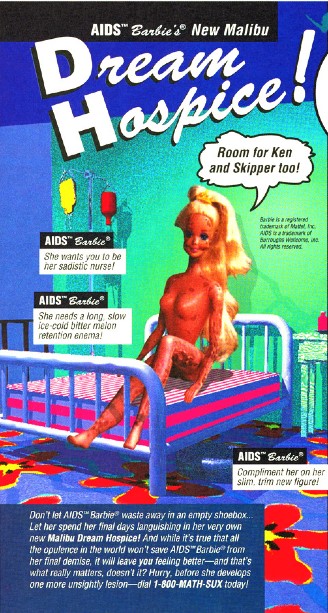
I came across recently a sardonic, humorously bizarre little zine in the Beowulf Thorne papers (GLBT Historical Society, 2003-10) called Diseased Pariah News (DPN). DPN was a zine created during the early 90’s that used gallows humor to humorously educate/entertain mostly gay (often white) cisgender men about HIV/AIDS among other gay men’s health issues. Humor is not something I would immediately associate with AIDS/HIV. Certainly, in the popular imagination AIDS and humor couldn’t be further apart. Queer white, cis, men living with HIV/AIDS in popular media depictions are generally akin to Tom Hanks in Philadelphia: a “noble, suffering AIDS victim”.
Further, many current LGBTQ media consumers tend to shy away from LGBTQ depictions that have overt internalized homophobia/transphobia, straying away from media depictions that might seem to make light of oppressive circumstances in ways that are ultimately self- cannibalizing. Rupaul was famously castigated for having content on her show that was deemed transphobic. Lisa Lampanelli, though not queer, is known for her gallows humor and recently left show business citing, “people in their 20s and 30s weren’t getting into that [insult comedy] tradition”. I spoke to a friend on Facebook about DPN and they echoed a popularly resonant sentiment, “I really don’t like to view historical media/works of art relating to our [queer] community. Because they always carry the hint of shame, of internalized homophobia and transphobia.”
Clearly, we are currently living through a shift in what we find humorous from particular groups of people based on their identities. And to be honest, it shouldn’t be ok for a white, cisgender, straight, man or woman to make jokes about communities that they historically (or contemporaneously, for that matter) oppress. But should queer people with HIV/AIDS be able to laugh at their own lived experiences? If observational comedy is about illuminating the mundane and often untintentionally humorous aspects of our everyday lives then DPN represents to me a group of queers with HIV/AIDS taking this to its’ logical conclusion: finding humor in the everyday lives of queer folx living with HIV/AIDS. Additionally, I think something is foreclosed when we as a queer community rush to quash inter-group humor that may on its surface appear aberrant. Queer people should be able to laugh at their own lived experiences if they so desire, especially, if by laughing, we find a form of resistance while skewering social and political realities that we ultimately find empowering.
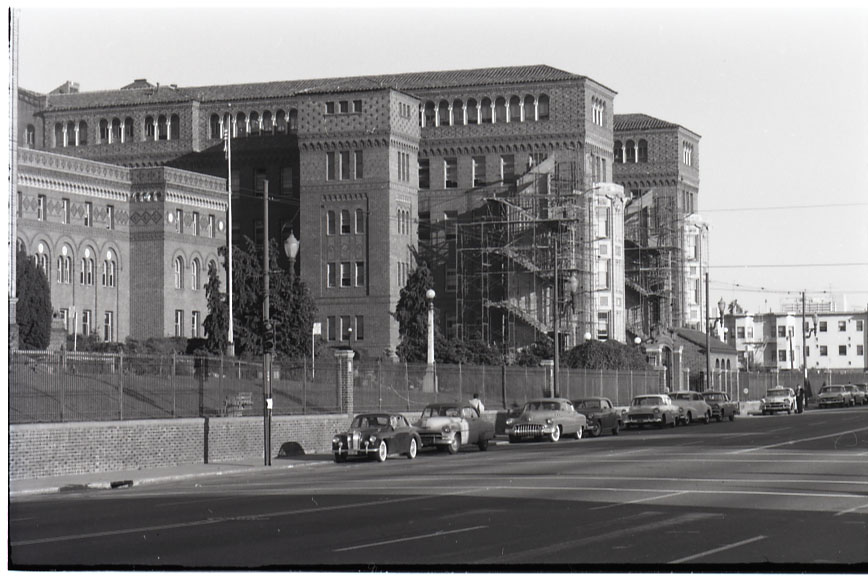
We are excited to announce a new collection from the ZSFG Archives. The Longenecker Photograph Collection, consisting of twelve boxes of prints, negatives, and glass plate negatives, is now available for research.
Don S Longenecker was the official photographer for San Francisco General Hospital from the 1950s to the 1980s. During that time, he took photos of the interiors and exteriors of the hospital campus, staff, events, and patients, including portraits of staff members and medical photos of patients for use in publications.
ZSFG interns and residents, June 1959
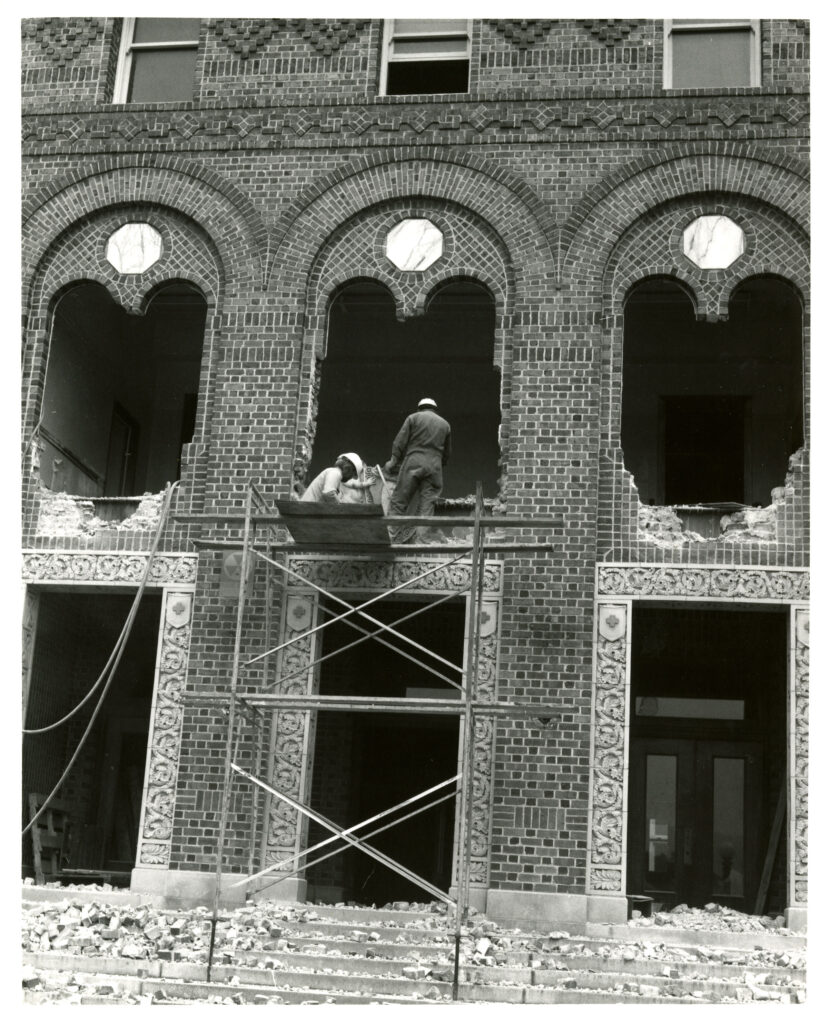
Of particular note are the images that document the many changes to the hospital campus during the 30+ years of Longenecker’s career. For example, the collection features images of the addition of fire escapes to the Nightingale wards of Buildings 10, 20, 30, and 40, the demolition of the old administration building that originally stood at the front gate entrance to the hospital, and the dedication of the new pathology building in 1967, along with other photos of both interior and exterior remodeling and construction. The collection also includes detailed images of the brickwork and architecture of the historic buildings that date back to 1915.
Adding fire escapes to Buildings 30 and 40, circa 1950s.During demolition of the administration building, circa 1960s.
Other highlights of the collection include photos of the surgical amphitheater, Mission Emergency, the dedication of the Trauma Center, staff labor strikes, hospital equipment, and many photos of staff events and celebrations.